PVC Mapping and Ablation
Definition
Catheter-based localisation and ablation of premature ventricular complexes (PVCs), now established as a first-line therapy for symptomatic PVCs, PVC-induced cardiomyopathy, and PVC-triggered ventricular fibrillation. Accurate mapping of the anatomical site of origin is the prerequisite for successful ablation.
Key Concepts
Indications
- Symptomatic PVCs refractory to or intolerant of antiarrhythmic drugs (AADs); HRS Class I for RVOT, tricuspid/mitral annulus, AMC, moderator band, papillary muscle PVCs; Class IIa for LVOT, LV summit, parahisian region (sources/PVC-ablation-jaccep-2024, rating: high)
- PVC-induced cardiomyopathy: Class I/IIa (HRS); see concepts/PVC-Induced-Cardiomyopathy (sources/PVC-ablation-jaccep-2024)
- PVC-triggered VF (short-coupled VF): Class IIa; short-coupled PVCs (coupling interval <350 ms) from LV/RV Purkinje system account for 6.6–7.8% of aborted cardiac arrest; ablation freedom from VF ~89% (sources/PVC-ablation-jaccep-2024)
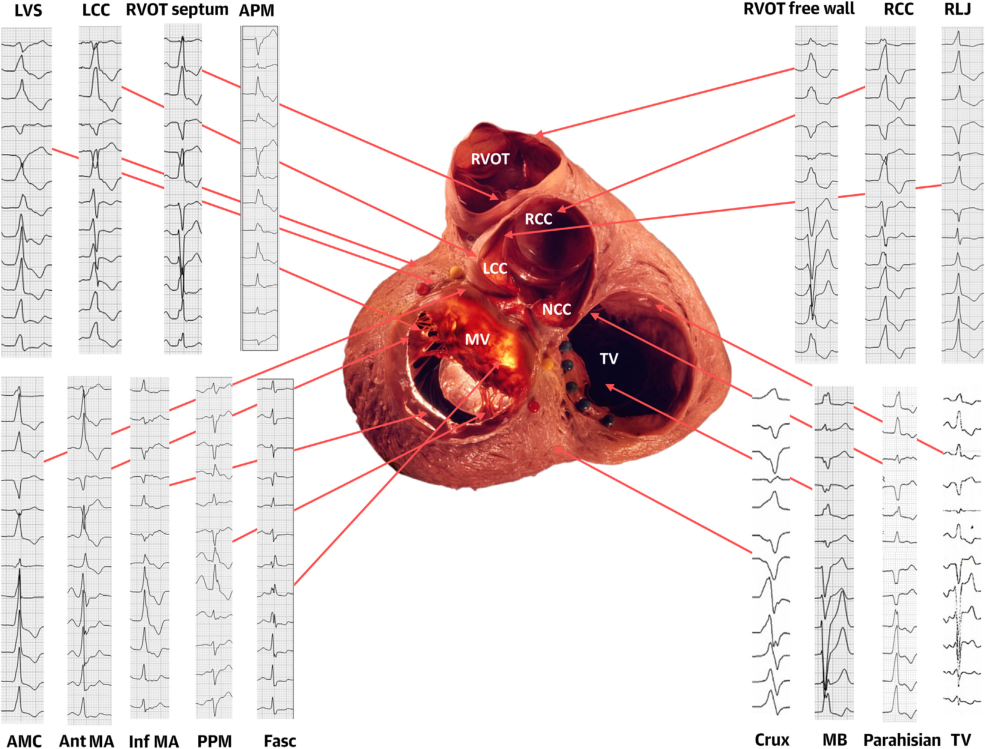
ECG Localisation
- Bundle branch block: RBBB pattern → LV origin; LBBB → RV or interventricular septum (sources/PVC-ablation-jaccep-2024)
- QRS duration: Narrow → septal; wide → free wall (sources/PVC-ablation-jaccep-2024)
- Axis: Inferior (positive II/III) → outflow tract or superior AV valves; superior → inferior ventricle (sources/PVC-ablation-jaccep-2024)
- Key site ECG signatures (sources/PVC-ablation-jaccep-2024):
| Site | Pattern | Key ECG Features |
|---|---|---|
| RVOT (septal) | LBBB, inferior axis | Transition V3–V4 |
| RVOT (free wall) | LBBB, inferior axis | Transition V4–V5, wider QRS, inferior notching |
| Pulmonary artery | LBBB, inferior axis | Larger R inferior, high aVL/aVR ratio |
| LCC | RBBB, inferior axis | Multiphasic QRS in V1 |
| AMC | RBBB, inferior axis | qR in V1 |
| Anterolateral mitral annulus | RBBB, inferior axis | Monomorphic R in V1 |
| LV summit (accessible) | RBBB, early transition | MDI >0.55, taller R in III vs II, V2 pattern break |
| LV summit (inaccessible) | LBBB, V2–V3 transition | Left superior axis |
| Parahisian | LBBB, V2–V3 transition | R in I/aVL, narrow QRS, lead II > III |
| Posteromedial papillary muscle | RBBB | Left or right superior axis, V3–V5 transition |
| Anterolateral papillary muscle | RBBB | Right inferior axis, inferior lead discordance |
| LV Purkinje | RBBB-like | Narrow QRS (<130 ms), rsR' in V1, initial Q in I |
| Moderator band | LBBB | Left superior axis, late transition >V4 |
| Basal crux | LBBB | Left superior axis, V2 transition, QS in inferior leads, MDI >0.55 |
 |
- RVOT vs LVOT differentiation algorithms — see concepts/OTVA-ECG-Localization for full algorithm tables and stepwise approach (sources/RVOT-LVOT-circ-ep-2019, rating: high)
- Best overall algorithm: Combined TZ index + V2S/V3R formula (Y = −1.15×TZ − 0.494×V2S/V3R; LVOT if ≥−0.76; Youden index 0.77; n=695) (sources/RVOT-LVOT-circ-ep-2019)
- Best for V3 precordial transition (38% of cases): V2S/V3R index ≤1.5 (sens 94%, spec 78% in V3 subgroup) or V3R/V7 index ≥0.85 (AUC 0.95, prospective accuracy 98.6%) (sources/RVOT-LVOT-circ-ep-2019)
- Key pitfall — preferential conduction: ~25% of aortic sinus OTVAs breakout earliest at the RVOT; excellent pacemap at RVOT but ablation fails; adjacent LVOT near-field signal is the true target (sources/RVOT-LVOT-circ-ep-2019)
Mapping Techniques
Activation Mapping
- Preferred when PVCs are present or inducible; target: earliest local activation >30 ms pre-QRS onset (sources/PVC-ablation-jaccep-2024)
- Multielectrode catheters (PentaRay, OctaRay, HD Grid, IntellaMap Orion) allow rapid high-resolution mapping
- Limitations: requires frequent spontaneous PVCs; risk of PVC suppression by catheter contact; far-field signal confusion (sources/PVC-ablation-jaccep-2024)
- Unipolar QS morphology also suggests earliest activation but lacks specificity for deep intramural foci (sources/PVC-ablation-jaccep-2024)
Pace Mapping
- Complementary technique; main strategy when intraprocedural PVC burden is low (sources/PVC-ablation-jaccep-2024)
- Match 11/12 or 12/12 leads visually; automated algorithms: PASO (CARTO), Score Map (Ensite)
- Spatial resolution 1.8 cm² (vs 1.2 cm² for activation mapping); exclusive pace mapping achieves ~79–80% clinical success (sources/PVC-ablation-jaccep-2024)
- Unreliable for fascicular/Purkinje PVCs (far-field capture of surrounding myocardium) (sources/PVC-ablation-jaccep-2024)
ECGI (Electrocardiographic Imaging)
- Noninvasive vest with body-surface electrodes + CT/CMR geometry (CardioInsight) (sources/PVC-ablation-jaccep-2024)
- 96% accuracy for outflow tract VAs; distance ~22.6 mm from true site in re-entrant VT
- Role: guiding stereotactic radioablation when catheter ablation has failed (sources/PVC-ablation-jaccep-2024)
Intramural Origin — Diagnostic Indicators
- Earliest endo/epicardial activation <−20 ms pre-QRS; similar timing across chambers (within 10 ms); diffuse early activation; earliest activation in septal coronary vein; suboptimal pace maps; late or transient PVC suppression (sources/PVC-ablation-jaccep-2024)
- Accounts for ~20% of LVOT PVCs and ~45% of suspected LV summit PVCs (sources/PVC-ablation-jaccep-2024)
Ablation Energy Sources
| Modality | Primary Use | Key Advantage | Limitation |
|---|---|---|---|
| RF (irrigated) | Standard; all sites | Versatile; adjustable power | Limited depth for intramural substrate |
| Cryoablation | Parahisian; papillary muscles | Reversible (−30°C); catheter stability via ice adherence | Longer application; larger catheter |
| Retrograde venous ethanol | LV summit; intramural septum | Reaches inaccessible intramural foci | Operator-dependent; balloon occlusion required |
| Stereotactic radioablation | Refractory/high-risk cases | Non-invasive; no vascular access needed | Limited PVC-specific data; complex logistics |
| Pulsed field ablation (PFA) | Emerging for VAs | Tissue-selective; no thermal injury | Very limited ventricular experience |
(sources/PVC-ablation-jaccep-2024)
Strategies for intramural PVC ablation (stepwise escalation) (sources/PVC-ablation-jaccep-2024):
- Extended RF applications (up to 5 min)
- Modified irrigation (half-normal saline or 5% dextrose → larger lesions)
- Impedance modulation (repositioning dispersive patch)
- Simultaneous unipolar ablation (2 catheters, separate generators)
- Bipolar ablation (active catheter to second catheter as return electrode)
- Retractable needle catheter
- Retrograde coronary venous ethanol ablation
- Stereotactic radioablation
Site-Specific Strategies
RVOT and Pulmonary Artery
- Retroflexed catheter approach; deflectable sheath; irrigated catheter 20–35 W; coronary angiogram before ablating above left pulmonary cusp (proximity to left main/LAD) (sources/PVC-ablation-jaccep-2024)
- ICE useful to confirm catheter position relative to pulmonary valve and identify myocardial sleeves extending into pulmonary artery (sources/PVC-ablation-jaccep-2024)
LV Ostium (Aortic Cusps, Subaortic LVOT, Mitral Annulus, AMC)
- Retrograde aortic access preferred; trans-septal (Agilis sheath) if aortic calcification or mechanical aortic valve (sources/PVC-ablation-jaccep-2024)
- Irrigated catheter 20–45 W; coronary angiogram mandatory for cusp/venous ablation (sources/PVC-ablation-jaccep-2024)
LV Summit
- If endocardium-to-earliest-epicardial distance <14 mm → endocardial ablation preferred; if >14 mm → coronary venous (GCV/AIV) ablation first (sources/PVC-ablation-jaccep-2024)
- Comprehensive mapping: GCV/AIV (epicardial) + septal perforator veins (intramural) + endocardial LVOT; retrograde venous ethanol as escalation (sources/PVC-ablation-jaccep-2024)
LV Papillary Muscles
- ICE essential for catheter-tissue contact and orientation; activation mapping + Purkinje potential targeting; cryoablation as RF bailout (enhanced stability) (sources/PVC-ablation-jaccep-2024)
LV Purkinje System
- Target earliest fascicular potential (FP), not earliest ventricular electrogram; retrograde aortic approach; map His/LBB/LAF/LPF; monitor AV conduction and QRS during RF (sources/PVC-ablation-jaccep-2024)
Parahisian Region
- Ablation within 10 mm of His electrogram — risk of AV block; systematic multi-structure mapping; target ≥5 mm from largest His potential; cryoablation if His visible at optimal site (sources/PVC-ablation-jaccep-2024)
Moderator Band and RV Papillary Muscles
- Common source of VF-triggering PVCs; Purkinje potential at successful site; multiple ablation points often needed; cryoablation advantageous for stability (sources/PVC-ablation-jaccep-2024)
Outcomes
- Large multicenter series (n=1,185): 84% acute success; 71% long-term freedom without AADs, 85% with AADs; RVOT origin = only independent predictor of success; major complications 2.4% (groin 1.3%, cardiac tamponade 0.8%, AV block 0.1%) (sources/PVC-ablation-jaccep-2024)
- Epicardial origin + multifocal PVCs = independent predictors of ablation failure (sources/PVC-ablation-jaccep-2024)
Contradictions / Open Questions
- No RCTs compare ablation strategies for specific PVC sites; all site-specific guidance is based on case series and expert opinion (sources/PVC-ablation-jaccep-2024)
- The appropriate escalation threshold from endocardial to venous/epicardial approaches for LV summit PVCs (currently guided by the 14 mm endocardium-to-epicardium distance rule) requires prospective validation (sources/PVC-ablation-jaccep-2024)
- Ventricular PFA is promising (tissue-selective, non-thermal) but lacks robust outcome data; its eventual role vs. RF for standard PVC sites is undefined (sources/PVC-ablation-jaccep-2024)
- ECGI accuracy for non-outflow-tract PVCs and re-entrant arrhythmias is insufficient to guide catheter ablation; its role is currently limited to pre-stereotactic radioablation planning (sources/PVC-ablation-jaccep-2024)
Connections
- Related to concepts/OTVA-ECG-Localization — comprehensive ECG algorithm reference for outflow tract PVCs
- Related to concepts/PVC-Induced-Cardiomyopathy
- Related to concepts/Pulsed-Field-Ablation — emerging ventricular PFA
- Related to concepts/Catheter-Ablation-AF — shared energy sources and mapping technology
- Related to concepts/Electrical-Storm — PVC-triggered VF management
- Related to entities/Idiopathic-Ventricular-Fibrillation — short-coupled PVC triggers