Heart Failure with Preserved Ejection Fraction (HFpEF)
Definition
HFpEF is defined by the presence of HF symptoms ± signs, LVEF ≥50%, and objective evidence of cardiac structural and/or functional abnormalities consistent with LV diastolic dysfunction/raised LV filling pressures, including raised natriuretic peptides. The greater the number of abnormalities present, the higher the likelihood of HFpEF. (sources/HF-ESC-2021, rating: very high)
Epidemiology
- HFpEF accounts for ~16% of outpatient HF in ESC Long-Term Registry; prevalence increases with age. (sources/HF-ESC-2021, rating: very high)
- Comorbidities (hypertension, obesity, T2DM, CKD, AF) are highly prevalent in HFpEF and drive pathophysiology. (sources/HF-ESC-2021, rating: very high)
- COPD and HFpEF: COPD is present in 14–34% of HFpEF hospital cohorts, 16% of RCT populations, and 14–34% of community/outpatient cohorts — higher prevalence than in other HF phenotypes. COPD is an independent prognostic risk factor: all-cause hospitalization RR 1.66 (95% CI 1.47–1.87), all-cause mortality RR 1.62 (95% CI 1.34–1.95), and post-discharge mortality RR 2.57 (95% CI 1.34–4.93). HF-caused hospitalization: RR 1.64. (sources/copd-hfpef-eschf-2025, rating: high)
- Obesity and HFpEF: HFpEF is more strongly associated with obesity than HFrEF. Overweight → 38% higher HFpEF risk; class 1 obesity → 56% higher HFpEF risk, independently of other CVD risk factors (Pandey et al., pooled analysis of 3 longitudinal studies). (sources/obesity-cv-aha-2021, rating: very high)
- Normal natriuretic peptide levels do not exclude HFpEF in obese patients — adipose tissue clears BNP, reducing measured levels even in the presence of elevated filling pressures. (sources/obesity-cv-aha-2021, rating: very high)
Pathophysiology
Comorbidity-Driven Mechanisms
- Systemic comorbidities (hypertension, obesity, T2DM, CKD, AF) promote coronary microvascular inflammation, cardiomyocyte hypertrophy, and interstitial fibrosis — the dominant pathophysiological substrate in HFpEF. (sources/HF-ESC-2021, rating: very high)
- COPD as comorbidity driver: COPD activates the same coronary microvascular endothelial inflammation pathway as other HFpEF comorbidities — systemic pro-inflammatory state → microvascular inflammation → cardiomyocyte hypertrophy + interstitial fibrosis. COPD additionally augments left ventricular diastolic dysfunction (LVDD) risk and creates a bidirectional cycle where elevated LV filling pressures worsen during COPD exacerbations. Hypoxia/bronchodilators cause tachycardia (shortened diastolic filling); bronchial obstruction reduces venous return; pericardial constraint further impairs LV function. Patients with COPD+HFpEF show greater arterial stiffness and LV fibrosis than single-disease patients. (sources/copd-hfpef-eschf-2025, rating: high)
- Increased cardiomyocyte passive stiffness is a hallmark of HFpEF, arising from both extracellular matrix changes and intrinsic sarcomeric protein modifications.
Obesity-HFpEF Phenotype
- Obesity produces a distinct HFpEF phenotype compared with non-obese HFpEF: greater concentric LV remodeling, RV dilatation and dysfunction, pericardial restraint, ventricular interdependence, and significantly lower exercise capacity. These features are driven by greater epicardial fat thickness and volume — the first study to formally characterize this as a distinct obesity-HFpEF pathophysiology. (sources/obesity-cv-aha-2021, rating: very high)
- Visceral adiposity → higher blood volume and cardiac output → LVH and LV diastolic dysfunction → HFpEF. Obesity also causes myocardial fat accumulation and fibrosis through epicardial adipose tissue paracrine signaling. (sources/obesity-cv-aha-2021, rating: very high)
- The H2FPEF score includes Obesity (BMI >30) as the highest-weighted component (2 of 9 points), reflecting the dominant role of obesity in HFpEF clinical probability. (sources/HF-AHA-2022, rating: very high)
- See entities/Obesity and concepts/Visceral-Adiposity for full mechanistic detail.
Titin Stiffness Mechanisms
- Titin contributes substantially to cardiomyocyte passive stiffness through multiple post-translational mechanisms. (sources/TTN-CVResearch-2022, rating: high)
- Isoform shift: Increased N2BA:N2B ratio observed in some HFpEF patients → lower titin-based stiffness as an apparent compensatory mechanism. The direction and functional significance remain inconsistent across studies. (sources/TTN-CVResearch-2022, rating: high)
- Phosphorylation: N2Bus hypo-phosphorylation (reduces extensibility) + PEVK hyper-phosphorylation (increases stiffness) → combined increase in passive stiffness. Both PKA/PKG-mediated N2Bus phosphorylation and the cGMP-PKG pathway are impaired in HFpEF. (sources/TTN-CVResearch-2022, rating: high)
- Acetylation: Reduced SIRT1 activity in HFpEF → increased titin acetylation → increased stiffness. NAD⁺/NAM treatment restores SIRT1 → deacetylation of titin spring → reduced stiffness in animal models. (sources/TTN-CVResearch-2022, rating: high)
- Failed clinical trials targeting titin phosphorylation via cGMP-PKG:
- RELAX (sildenafil/PDE5A inhibitor): no improvement in diastolic function or VO2 in HFpEF. (sources/TTN-CVResearch-2022, rating: high); (sources/HF-AHA-2022, rating: very high)
- VITALITY and SOCRATES (sGC stimulators): no improvement in HFpEF despite pre-clinical evidence of N2Bus phosphorylation increase and reduced cardiomyocyte stiffness. (sources/TTN-CVResearch-2022, rating: high)
- See concepts/Titin-PTMs and concepts/Titin-Isoform-Switch for full mechanistic detail.
Genetic and Infiltrative Causes
- Anderson–Fabry Disease (AFD): 40% of AFD patients meet ESC HF criteria; 91% of those have HFpEF (rather than HFrEF). Subclinical diastolic dysfunction may precede LVH — symptoms can appear before significant wall thickening. (sources/fabry-ehj-2024, rating: high)
- ATTR cardiac amyloidosis (ATTR-CA): Prevalence in HFpEF estimated at 5–13% (limited autopsy/nuclear screening data); one prospective biopsy study found 14% of HFpEF had cardiac amyloidosis, majority TTR type. (sources/echo-hfpef-ase-2025, rating: very high)
- See entities/Fabry-Disease, concepts/Fabry-Cardiomyopathy, and entities/ATTR-Amyloidosis for full detail.
Atrial Myopathy in HFpEF
- In HFpEF, mechanical atrial dysfunction (impaired LASr, elevated LAVi) is an independent and better predictor than AF for adverse clinical outcomes including morbidity (HF) and cardiovascular mortality. AF alone is insufficient to capture the full atrial risk in this population. (sources/atrial-cmp-esc-2025, rating: high)
- LASr correlates with histological atrial fibrosis in advanced HF patients, making echocardiographic LASr a surrogate measure of atrial fibrosis — relevant for both diagnosis and prognostication in HFpEF. (sources/atrial-cmp-esc-2025, rating: high)
- A subset of HFpEF is characterized by 'disproportionate LA myopathy' — LA dysfunction more pronounced than expected from LV dysfunction alone. Right heart dysfunction, enhanced left-to-right atrial interaction, and pericardial constraint may contribute. (sources/atrial-cmp-esc-2025, rating: high)
- The obesity-HFpEF phenotype features more atrial epicardial adipose tissue when AF co-occurs, contributing to atrial remodelling via paracrine fibrotic/inflammatory signalling. (sources/atrial-cmp-esc-2025, rating: high)
- This disproportionate LA myopathy may represent a distinct HFpEF phenotype or an early-stage manifestation of atrial failure — the distinction requires further study.
- See concepts/Atrial-Cardiomyopathy and concepts/Atrial-Failure for the full AtCM diagnostic framework.
Clonal Hematopoiesis (TET2)
- TET2-CH is 2.4-fold enriched in HFpEF — a gene-specific association not seen with the overall HFrEF/HFpEF classification, identifying CH as a potential contributor to HFpEF pathophysiology specifically. (sources/ch-aha-2026, rating: very high)
- Mechanism: TET2 loss-of-function → NLRP3 inflammasome overactivation → increased IL-1β secretion; elevated circulating IL-1β is unique to TET2-CH among all CH variants and is the likely mediator of the cardiac inflammatory phenotype. (sources/ch-aha-2026)
- CANTOS post-hoc: canakinumab (anti-IL-1β) reduced ischemic events far more in TET2-CH carriers — mechanistic relevance for HFpEF inflammatory phenotype under investigation. (sources/ch-aha-2026)
- See concepts/Clonal-Hematopoiesis for full gene-specific mechanisms, emerging therapeutic strategies, and the broader CH–HF risk association (25% overall HF risk increase in CH carriers).
Diagnosis
LVEF-Based Phenotype Classification
- HFpEF is one of three LVEF-based HF phenotypes: HFrEF (LVEF ≤40%), HFmrEF (LVEF 41–49%), HFpEF (LVEF ≥50%). (sources/HF-ESC-2021, rating: very high)
- The 2023 ESC task force considered renaming HFpEF to HFnEF (normal EF) but retained current terminology, deferring to the next full guideline update. (sources/HF-update-ESC-2023, rating: very high)
- In clinical trials (EMPEROR-Preserved, DELIVER): NT-proBNP thresholds used were >300 pg/mL for sinus rhythm and >900 pg/mL for AF. These thresholds were not mandated in the 2023 recommendation. (sources/HF-update-ESC-2023, rating: very high)
Guideline Definitions: ESC vs ACC/AHA
- ACC/AHA: LVEF ≥50% + symptoms/signs + evidence of diastolic dysfunction. (sources/echo-hfpef-ase-2025, rating: very high)
- ESC: LVEF ≥50% + symptoms/signs + elevated natriuretic peptides + at least one of:
- Structural: LAVi >34 mL/m² or LVMi ≥115/95 g/m² (men/women)
- Functional: E/e' ≥13 or mean e' <9 cm/s (sources/echo-hfpef-ase-2025, rating: very high)
- Up to 30% of HFpEF patients can have normal NP levels (particularly obese patients) — normal NP does not exclude HFpEF. (sources/echo-hfpef-ase-2025, rating: very high)
HFpEF Prediction Scores
- H2FPEF Score (0–9): Discriminates HFpEF from noncardiac dyspnoea. Components: Heavy (obesity, BMI >30; 2 pts), Hypertensive (≥2 antihypertensives; 1 pt), Atrial fibrillation (3 pts), Filling pressure (E/e' >9; 1 pt), Elderly (age >60 years; 1 pt), Pulmonary hypertension (PASP >35 mmHg; 1 pt). Each 1-unit increase doubles odds of HFpEF (OR 1.98; c-statistic 0.841). (sources/HF-AHA-2022, rating: very high)
- Score <2 = low likelihood; 2–5 = intermediate (40–80%); ≥6 = high likelihood
- Intermediate scores: refer for exercise echocardiography or invasive hemodynamics
- HFA-PEFF Algorithm (ESC): Stepwise pretest probability → comprehensive echo + NP score → exercise/invasive testing if intermediate. (sources/echo-hfpef-ase-2025, rating: very high)
- The 2025 ASE guideline formally incorporates both H2FPEF and HFA-PEFF into HFpEF diagnostic workup for patients with uncertain probability. (sources/echo-hfpef-ase-2025, rating: very high)
ASE 2025 — Stepwise Echocardiographic Diagnosis Algorithm
Comprehensive stepwise algorithm from the 2025 ASE guideline update: (sources/echo-hfpef-ase-2025, rating: very high)
- History, physical, CXR, labs, natriuretic peptides → exclude non-cardiac dyspnea
- Comprehensive echo → exclude: significant valvular disease (MS/primary MR/AS/AR/TR), significant CAD, non-cardiac PH, cardiac amyloidosis, HCM, pericardial constriction
- Apply LAP estimation algorithm (e', E/e', TR velocity/PASP as primary variables)
- If LAP elevated → HFpEF confirmed
- If LAP normal → diastolic exercise echo (or RHC with/without exercise)
- If exercise echo positive → HFpEF confirmed; if negative → non-cardiac dyspnea; if inconclusive → RHC
RHC gold standard: Rest mean PCWP >15 mmHg or exercise mean PCWP ≥25 mmHg (end-expiration) confirms HFpEF. (sources/echo-hfpef-ase-2025, rating: very high)
Definition of LV Diastolic Dysfunction (ASE 2025 Two-Step Algorithm)
A two-step approach is used to define the presence of LV diastolic dysfunction. (sources/echo-hfpef-ase-2025, rating: very high)
Step 1 — Assess impaired LV relaxation (e' velocity):
- Reduced e' defined as: septal e' ≤6 cm/s OR lateral e' ≤7 cm/s OR average e' ≤6.5 cm/s
Step 2 — Assess LA/LV remodeling and elevated LAP (≥1 marker required):
| Marker | Abnormal Threshold |
|---|---|
| Average E/e' | >14 |
| LA reservoir strain (LARS) | ≤18% |
| E/A ratio | ≤0.8 (age-adjusted) OR ≥2 |
| LAVi | >34 mL/m² |
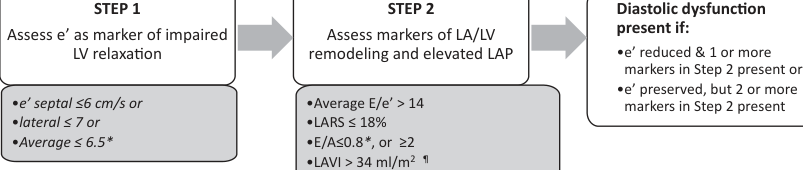
Diagnostic rule:
- Diastolic dysfunction present if: reduced e' + ≥1 Step 2 marker, OR normal e' + ≥2 Step 2 markers
- Additional supportive finding: LV mass index >115 g/m² (men) or >95 g/m² (women), excluding athletes
Key change from 2016 guideline: LAVi demoted from primary to secondary variable in the LAP estimation algorithm — poor correlation with acute LAP changes and multiple non-diastolic causes of LA enlargement (AF, MR, high-output states). LARS (≤18%) elevated to primary parameter with high specificity for elevated LAP. (sources/echo-hfpef-ase-2025, rating: very high)
Echocardiographic HFpEF Features
- Typical features: LV hypertrophy, concentric remodeling, LA enlargement, diastolic dysfunction (Grade 2 or 3), reduced LV GLS, reduced LARS — but none are individually diagnostic. (sources/echo-hfpef-ase-2025, rating: very high)
- See concepts/LV-Diastolic-Function for the full LAP estimation algorithm and diastolic dysfunction grading.
Diastolic Exercise Echocardiography
- Up to 50% of HFpEF patients have normal resting LAP that rises only with exercise — exercise echo is essential in this phenotype. (sources/echo-hfpef-ase-2025, rating: very high)
- Positive (definite abnormal): Average E/e' ≥14 (or septal ≥15) AND peak TR velocity >3.2 m/s during exercise. (sources/echo-hfpef-ase-2025, rating: very high)
- Likely HFpEF: E/e' >14 + TR velocity >2.8 but <3.2 m/s. (sources/echo-hfpef-ase-2025, rating: very high)
- Normal: Average E/e' <10 AND TR velocity <2.8 m/s. (sources/echo-hfpef-ase-2025, rating: very high)
Management
Historical Pharmacotherapy (Pre-SGLT2i Era)
- As of 2021 ESC guidelines: no pharmacotherapy shown to reduce mortality in HFpEF. ACE-I, ARB (CHARM-Preserved, I-PRESERVE), ARNI (PARAGON-HF P=0.06), and MRA (TOPCAT HR 0.89 P=0.14) all failed primary composite endpoints — though TOPCAT HF hospitalisation was significantly reduced (HR 0.83; P=0.04). (sources/HF-ESC-2021, sources/spironolactone-hfpef-topcat-nejm-2014, rating: very high)
- Treatment focused on managing aetiologies and comorbidities, and symptom relief with diuretics. (sources/HF-ESC-2021, rating: very high)
ARNI (Sacubitril–Valsartan) — PARAGON-HF
- PARAGON-HF (Solomon et al., 2019, NEJM; n=4,796; LVEF ≥45%; sacubitril–valsartan vs. valsartan; median 35 months): The primary composite of total HF hospitalisations + CV death did not reach statistical significance (RR 0.87, 95% CI 0.75–1.01; P=0.06). (sources/arni-paragon-hf-nejm-2019, rating: very high)
- HF hospitalisations (RR 0.85, 95% CI 0.72–1.00) and CV death (HR 0.95, 95% CI 0.79–1.16) were both non-significant individually. (sources/arni-paragon-hf-nejm-2019, rating: very high)
- Meaningful secondary signals (exploratory after primary not met):
- NYHA class improvement at 8 months: 15.0% vs. 12.6% (OR 1.45, 95% CI 1.13–1.86)
- Worsening renal function halved: 1.4% vs. 2.7% (HR 0.50, 95% CI 0.33–0.77)
- KCCQ clinical summary score: +1.0 point improvement (95% CI 0.0–2.1) (sources/arni-paragon-hf-nejm-2019, rating: very high)
- Subgroup signals: Pre-specified analysis suggested possible differential benefit in patients with LVEF 45–57% (lower EF boundary, overlapping HFmrEF) and in women. These are hypothesis-generating only. (sources/arni-paragon-hf-nejm-2019, rating: very high)
- Guideline position: AHA 2022 COR 2b, LOE B-R — "particularly in those with lower LVEF"; ESC 2023 does not formally recommend ARNI in HFpEF (SGLT2i received Class I, Level A instead). (sources/HF-AHA-2022, rating: very high)
MRA (Spironolactone) — TOPCAT
- TOPCAT (Pitt/Pfeffer et al., NEJM 2014; n=3,445; LVEF ≥45%; 233 sites; 6 countries; 1:1 double-blind; NHLBI-funded; mean 3.3 years): Primary composite (CV death + aborted arrest + HF hospitalisation): HR 0.89 (95% CI 0.77–1.04; P=0.14) — NOT significant. CV death HR 0.90 (NS); all-cause death HR 0.91 (NS). HF hospitalisation: HR 0.83 (95% CI 0.69–0.99; P=0.04) — significant. Total (including recurrent) HF hospitalisations: 394 vs 475 (P=0.03). (sources/spironolactone-hfpef-topcat-nejm-2014, rating: high)
- Stratum interaction (P=0.01): Hospitalisation-stratum (71.5%): HR 1.01 (P=0.92) — no benefit. BNP-stratum (28.5%; BNP ≥100 or NT-proBNP ≥360): HR 0.65 (95% CI 0.49–0.87; P=0.003) — significant benefit. BNP-stratum patients less likely to be from Russia/Georgia. (sources/spironolactone-hfpef-topcat-nejm-2014, rating: high)
- Regional post-hoc: Americas (US, Canada, Brazil, Argentina): 27.3% vs 31.8% (benefit visible); Russia/Georgia: 9.3% vs 8.4% (near-identical, no room to reduce). Americas-only primary HR ~0.82 (P=0.026). (sources/spironolactone-hfpef-topcat-nejm-2014, rating: high)
- Safety: Hyperkalemia doubled (18.7% vs 9.1%); creatinine doubling (10.2% vs 7.0%); hypokalemia reduced (16.2% vs 22.9%); ~34% discontinued drug. Frequent K/creatinine monitoring required. (sources/spironolactone-hfpef-topcat-nejm-2014, rating: high)
- Guideline position: AHA 2022 COR 2b, LOE B-R; ESC Class IIb — particularly at lower LVEF spectrum. Not Class I due to neutral primary endpoint (with the Russia/Georgia data integrity caveat). (sources/HF-AHA-2022, rating: very high)
Nonsteroidal MRA (Finerenone) — FINEARTS-HF (NEJM 2024)
- FINEARTS-HF (Solomon, McMurray et al., NEJM 2024; n=6,001; 654 sites; 37 countries; median 32 months; Bayer-funded): First MRA to achieve a significant primary endpoint in HFmrEF/HFpEF. Finerenone vs placebo in addition to usual therapy in patients with LVEF ≥40%.
- Primary composite (total worsening HF events + CV death): Rate ratio 0.84 (95% CI 0.74–0.95; P=0.007) — driven by HF events. (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high)
- Total worsening HF events: Rate ratio 0.82 (95% CI 0.71–0.94; P=0.006) — significant. (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high)
- CV death: HR 0.93 (95% CI 0.78–1.11) — NOT significant. (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high)
- All-cause death: HR 0.93 (95% CI 0.83–1.06) — NOT significant. (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high)
- KCCQ total symptom score: Difference +1.6 points (P<0.001) — statistically significant but below 5-point MCID. NYHA class improvement non-significant (OR 1.01). (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high)
- Kidney composite: HR 1.33 (95% CI 0.94–1.89) — NOT significant; numerically worse (opposite to CKD-T2DM trials). (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high)
- Safety: Hyperkalemia (K+ >6.0 mmol/L) 3.0% vs 1.4%; no hyperkalemia deaths; hypokalemia reduced. (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high)
- Key feature: Benefit consistent in patients on SGLT2i at baseline — suggesting complementary mechanism to SGLT2i. Subgroup results consistent across all 17 prespecified subgroups including LVEF <60% vs ≥60%. (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high)
Beta-Blockers in HFpEF+COPD — Avoid
- β-blockers are not recommended in HFpEF and are potentially detrimental (impair chronotropic reserve, worsen exercise tolerance). In the presence of coexisting COPD, this hazard is amplified. (sources/hf-copd-hfreview-2025, rating: high)
- Existing β-blockers should be discontinued in HFpEF+COPD (unless required for non-HF indication: angina, AF) to improve functional capacity and avoid respiratory side effects. (sources/hf-copd-hfreview-2025, rating: high)
- This contrasts sharply with HFrEF+COPD, where β-blockers remain Class I and bisoprolol reduces both HF events and COPD exacerbations. (sources/hf-copd-hfreview-2025, rating: high)
SGLT-2 Inhibitors — Dual Benefit in COPD+HFpEF
- In HFpEF patients with comorbid COPD, SGLT2 inhibitors may provide dual benefit: reducing HF hospitalizations (ESC 2023 Class I, Level A) and additionally reducing incident COPD and severe COPD exacerbations. Proposed mechanism: glucosuric effect → ↓serum glucose → ↓endogenous CO2 production → facilitates CO2 clearance in patients with CO2 retention. (sources/copd-hfpef-eschf-2025, rating: high)
ESC 2023 — SGLT2 Inhibitors (Class I, Level A)
- EMPEROR-Preserved (Anker, Packer et al., NEJM 2021; n=5,988; LVEF >40%; NYHA II–IV; ~50% T2DM; ~50% eGFR <60; median LVEF 54%; 622 centres; 23 countries; median 26.2 months; Boehringer Ingelheim/Eli Lilly-funded): Empagliflozin 10 mg OD vs placebo. First large pharmacotherapy trial with a statistically significant positive primary outcome in HFpEF — ending two decades of failed trials in this population. Primary composite (CV death or first HF hospitalisation): HR 0.79 (95% CI 0.69–0.90; P<0.001; NNT=31). HF hospitalisation component: HR 0.71 (95% CI 0.60–0.83). CV death: HR 0.91 (95% CI 0.76–1.09) — not significant. All-cause death: HR 1.00 — completely neutral. Total (first + recurrent) HF hospitalisations: HR 0.73 (P<0.001). eGFR decline: −1.25 vs −2.62 mL/min/1.73m²/year (P<0.001). Benefit consistent across prespecified LVEF subgroups (thresholds 50% and 60%) and with/without T2DM. Safety: genital/urinary tract infections and hypotension more frequent with empagliflozin; serious AE burden lower overall. (sources/empagliflozin-hfpef-nejm-2021, rating: very high; sources/HF-update-ESC-2023, rating: very high)
- DELIVER (dapagliflozin, n=6263, LVEF >40%, including improved LVEF, median 2.3 years): Primary composite of worsening HF or CV death reduced: HR 0.82 (95% CI 0.73–0.92; P<0.001). Worsening HF significantly reduced (HR 0.79, 95% CI 0.69–0.91); CV death not significantly reduced (HR 0.88, 95% CI 0.74–1.05). Total event burden reduced (rate ratio 0.77; P<0.001). KCCQ total symptom score improved (win ratio 1.11; mean +2.4 points vs placebo). Benefit consistent across full LVEF spectrum including LVEF ≥60% (no heterogeneity; contrasts with EMPEROR-Preserved signal of attenuation at ≥65%), in patients with/without T2DM, enrolled during/after hospitalization, and in those with previously reduced LVEF improved to >40% (HFrecEF subgroup). Safety similar to placebo. (sources/dapagliflozin-deliver-nejm-2022, rating: very high; sources/HF-update-ESC-2023, rating: very high)
- Pooled meta-analysis: 20% reduction in CV death or first HF hospitalization (HR 0.80; P<0.001); 26% reduction in HF hospitalization (HR 0.74; P<0.001). CV death not significantly reduced (HR 0.88; P=0.052). (sources/HF-update-ESC-2023, rating: very high)
- 2023 Recommendation: SGLT2 inhibitor (dapagliflozin or empagliflozin) Class I, Level A to reduce risk of HF hospitalization or CV death. Benefit independent of T2DM status. (sources/HF-update-ESC-2023, rating: very high)
- ESC 2023 Algorithm — Class I: Diuretics for fluid retention; SGLT2 inhibitor; treatment of aetiology, CV and non-CV comorbidities. Management remains heavily comorbidity-directed (AF, hypertension, diabetes, obesity, CKD, sleep apnoea). (sources/HF-update-ESC-2023, rating: very high)
SGLT2 Inhibitors in HFmrEF
- HFmrEF (LVEF 41–49%): SGLT2 inhibitors upgraded to Class I, Level A (from Class IIb/no recommendation in 2021). Evidence base is the same two trials (EMPEROR-Preserved and DELIVER enrolled LVEF >40%). (sources/HF-update-ESC-2023, rating: very high)
- In HFmrEF, other agents (ACE-I/ARNI/ARB, beta-blocker, MRA) remain Class IIb based on subgroup analyses; diuretics remain Class I for fluid retention. (sources/HF-update-ESC-2023, rating: very high)
- SGLT2 inhibitors should be considered in AFD-related HFpEF per ESC Class I recommendation; they may also confer additional renal benefit in AFD nephropathy. (sources/fabry-ehj-2024, rating: high)
- Cardiac myosin inhibitors (mavacamten) must not be used in AFD-HFpEF — approved only for sarcomeric obstructive HCM. (sources/fabry-ehj-2024, rating: high)
AHA 2022 — Pharmacotherapy (COR Levels)
- BP control: COR 1, LOE C-LD — titrate to published BP targets. (sources/HF-AHA-2022, rating: very high)
- SGLT2i: COR 2a, LOE B-R — beneficial for HF hospitalizations and CV mortality (EMPEROR-Preserved). (sources/HF-AHA-2022, rating: very high)
- AF management: COR 2a, LOE C-EO — useful for symptom improvement. (sources/HF-AHA-2022, rating: very high)
- MRA: COR 2b, LOE B-R — particularly at lower LVEF spectrum. TOPCAT: primary composite HR 0.89 (NS); HF hospitalisation HR 0.83 (P=0.04); BNP-stratum HR 0.65 (P=0.003); Americas-only HR ~0.82; Russia/Georgia data integrity confounds overall result. (sources/spironolactone-hfpef-topcat-nejm-2014, sources/HF-AHA-2022, rating: high–very high)
- ARB: COR 2b, LOE B-R — particularly at lower LVEF (CHARM-Preserved data). (sources/HF-AHA-2022, rating: very high)
- ARNi: COR 2b, LOE B-R — particularly at lower LVEF (PARAGON-HF subgroup). (sources/HF-AHA-2022, rating: very high)
- Nitrates and PDE5 inhibitors: COR 3 No Benefit, LOE B-R — routine use ineffective. NEAT-HFpEF: no improvement in activity tolerance with isosorbide mononitrate. RELAX: no improvement in VO2 or exercise tolerance with sildenafil. (sources/HF-AHA-2022, rating: very high)
Guideline Discordance: AHA 2022 vs ESC 2023 on SGLT2i
- AHA 2022: SGLT2i COR 2a — based solely on EMPEROR-Preserved. Published May 2022, before DELIVER (August 2022). (sources/HF-AHA-2022, rating: very high)
- ESC 2023: SGLT2i Class I, Level A — incorporates both EMPEROR-Preserved and DELIVER plus pooled meta-analysis. (sources/HF-update-ESC-2023, rating: very high)
- Both guidelines agree SGLT2i is beneficial in HFpEF; the difference in classification strength reflects publication timing, not disagreement on efficacy.
GLP-1 Receptor Agonist (Semaglutide) — STEP-HFpEF (NEJM 2023)
- STEP-HFpEF (Kosiborod, Borlaug et al., NEJM 2023; n=529; LVEF ≥45%; BMI ≥30; no diabetes; 96 sites; 13 countries; 52 weeks; Novo Nordisk-funded): First pharmacologic trial to specifically target obesity as a therapeutic strategy in HFpEF.
- Dual primary endpoints (both P<0.001):
- KCCQ-CSS: estimated difference +7.8 points (95% CI 4.8–10.9) — 4–15× larger than prior HFpEF pharmacotherapy trials (SGLT2i/ARNI/spironolactone: 0.5–2.3 points)
- Body weight: estimated difference −10.7 percentage points (95% CI −11.9 to −9.4)
- Confirmatory secondary endpoints (all P<0.001):
- 6MWT: +20.3m (95% CI 8.6–32.1) — greater than HF-ACTION exercise training benefit in HFrEF; comparable to HFpEF exercise training trials
- Hierarchical composite (death/HF events/KCCQ/6MWT): win ratio 1.72 (95% CI 1.37–2.15)
- CRP: −43.5% vs −7.3% (treatment ratio 0.61) — robust anti-inflammatory effect
- Exploratory: HF hospitalizations 1 vs 12 (HR 0.08; not powered); NT-proBNP fell despite weight loss (suggesting hemodynamic benefit beyond weight reduction alone)
- Safety: Serious adverse events 13.3% vs 26.7% (P<0.001) — approximately half the rate; driven by 4× fewer cardiac events (2.7% vs 11.3%); GI AEs led to more semaglutide discontinuations (35 vs 14) but discontinuation due to serious AEs was equal (6 vs 6)
- Current guideline status: Not yet incorporated into AHA 2022 or ESC 2023/2024 guidelines (trial published August 2023 after the ESC HF update). Expected to receive recommendation in next guideline update cycle for the obesity-HFpEF phenotype.
(sources/semaglutide-stephfpef-nejm-2023, rating: very high)
Dual GIP/GLP-1 Receptor Agonist (Tirzepatide) — SUMMIT (NEJM 2025)
- SUMMIT (Packer, Zile, Borlaug et al., NEJM 2025; n=731; LVEF ≥50%; BMI ≥30; NYHA II–IV; 129 centres; 9 countries; median 104 weeks; Eli Lilly-funded): First trial to demonstrate significant reduction in hard cardiovascular outcomes in obesity-HFpEF, with two prospectively designated primary endpoints both met.
- NT-proBNP not mandated for entry — key design distinction recognising that adiposity suppresses natriuretic peptides in obese HFpEF; median baseline NT-proBNP <200 pg/mL.
- Primary endpoint 1 — CV death or worsening HF (time-to-first event): 36 (9.9%) vs 56 (15.3%); HR 0.62 (95% CI 0.41–0.95; P=0.026)
- Worsening HF events: HR 0.54 (95% CI 0.34–0.85)
- Worsening HF requiring hospitalisation: HR 0.44 (95% CI 0.22–0.87)
- CV death: HR 1.58 (95% CI 0.52–4.83) — NS; numerically higher with tirzepatide; underpowered
- Primary endpoint 2 — KCCQ-CSS at 52 weeks: Between-group difference +6.9 pts (95% CI 3.3–10.6; P<0.001)
- Key secondary endpoints (all P<0.001): Weight −13.9% vs −2.2% (difference −11.6pp); 6MWT +18.3m; CRP −38.8% vs −5.9%
- All-cause death: HR 1.25 (95% CI 0.63–2.45) — NS; 19 tirzepatide vs 15 placebo; numerically higher; trial underpowered for mortality
- GI discontinuations: 4.1% tirzepatide vs 0% placebo; overall serious adverse events similar
- Benefit consistent across prespecified subgroups including NT-proBNP <200 pg/mL — suggests tirzepatide benefits low-NP obesity-HFpEF, challenging a requirement for elevated natriuretic peptides to initiate treatment
(sources/tirzepatide-hfpef-summit-nejm-2025, rating: very high)
Contradictions / Open Questions
- TOPCAT Russia/Georgia data integrity — the primary endpoint is unreliable: Post-hoc metabolite analysis (Pfeffer et al. 2015, Circulation) found spironolactone metabolite canrenone in only ~38% of Russian "active treatment" participants vs >90% in the Americas, strongly suggesting widespread dispensing of placebo in both arms in Russia/Georgia. The anomalously low placebo event rate in Russia/Georgia (8.4% vs 31.8% in the Americas) is consistent with these patients either not having genuine HFpEF or receiving placebo regardless of assignment. When Russia/Georgia data are excluded, the primary composite shows benefit (Americas HR ~0.82; P=0.026) and the stratum heterogeneity resolves. This data integrity problem is the principal reason for the neutral overall primary endpoint and explains why MRA earned only COR 2b/Class IIb rather than a stronger recommendation. Without this problem, TOPCAT might have shown significant benefit — making MRA a stronger candidate for HFpEF treatment. (sources/spironolactone-hfpef-topcat-nejm-2014, rating: high)
- TOPCAT stratum heterogeneity — two different HFpEF populations enrolled: The BNP stratum showed significant benefit (HR 0.65; P=0.003) while the hospitalisation stratum showed no benefit (HR 1.01; P=0.92). This interaction (P=0.01) may reflect genuine biological differences between patients entering via biochemical evidence of HF (more reliable HFpEF diagnosis) vs. those entering via prior hospitalisation alone (potentially more heterogeneous, easier to fabricate in Russia/Georgia). BNP-stratum patients had higher creatinine and lower eGFR — suggesting a more volume-overloaded, MRA-responsive phenotype. (sources/spironolactone-hfpef-topcat-nejm-2014, rating: high)
- PARAGON-HF: near-miss or true negative? The primary endpoint P=0.06 (alpha 0.048) raises the question of whether a different trial design — placebo comparator (valsartan has ARB activity), different LVEF threshold, or larger sample — would have reached significance. The effect size (RR 0.87) mirrors other near-miss HFpEF trials. The active comparator (valsartan) may have attenuated the true ARNI vs placebo difference, given CHARM-Preserved ARB signal. (sources/arni-paragon-hf-nejm-2019, rating: very high)
- ARNI subgroup signal (LVEF 45–57%) vs. SGLT2i across full EF range: PARAGON-HF suggests possible ARNI benefit at the lower EF boundary of HFpEF. EMPEROR-Preserved and DELIVER show SGLT2i benefit across the full LVEF spectrum (>40%). This creates a tension: is ARNI complementary to SGLT2i in lower-EF HFpEF, or does the SGLT2i Class I recommendation make ARNI COR 2b practically irrelevant? No head-to-head or combination trial data exist. (sources/arni-paragon-hf-nejm-2019, rating: very high; sources/HF-update-ESC-2023, rating: very high)
- Mechanical atrial dysfunction vs. AF in HFpEF: ESC/HFA 2025 AtCM consensus shows mechanical atrial dysfunction is a better predictor than AF in HFpEF — yet HFpEF management frameworks (AHA/ESC) continue to rely heavily on AF detection as a primary driver of management decisions (NT-proBNP thresholds, OAC, rate/rhythm control). This tension suggests atrial structural markers may need formal incorporation into HFpEF diagnostic and management algorithms. (sources/atrial-cmp-esc-2025, rating: high; sources/echo-hfpef-ase-2025, rating: very high)
- SGLT2i reduces HF hospitalizations but not CV death in HFpEF: Both EMPEROR-Preserved and DELIVER showed no significant reduction in CV death individually; the pooled meta-analysis also showed a non-significant trend (HR 0.88, P=0.052). The Class I, Level A recommendation rests on the composite endpoint driven by hospitalizations. The lower CV death rate in HFpEF vs. HFrEF (3.8 vs. 7.9 events/100 patient-years in DELIVER vs. DAPA-HF) means neither trial was powered for mortality alone. (sources/dapagliflozin-deliver-nejm-2022, rating: very high; sources/HF-update-ESC-2023, rating: very high)
- Improved EF phenotype (HFrecEF): DELIVER included patients with LVEF previously ≤40% that had improved to >40%. Dapagliflozin showed consistent benefit in this subgroup — suggesting SGLT2i may benefit "recovered EF" HF, but guideline classification of this subgroup remains undefined. (sources/dapagliflozin-deliver-nejm-2022, rating: very high; sources/HF-update-ESC-2023, rating: very high)
- Full EF spectrum benefit vs. EMPEROR-Preserved heterogeneity: DELIVER found no evidence of attenuation at LVEF ≥60% (consistent benefit across entire EF range), whereas EMPEROR-Preserved suggested possible attenuation at LVEF ≥65%. This discordance between the two pivotal SGLT2i HFpEF trials at the highest EF range remains unresolved — it may reflect trial design differences, or true biological uncertainty at normal EF. (sources/dapagliflozin-deliver-nejm-2022, rating: very high)
- EMPEROR-Preserved: all-cause death HR 1.00 — no mortality benefit whatsoever: The perfectly neutral all-cause mortality result (HR 1.00; 95% CI 0.87–1.15) in EMPEROR-Preserved contrasts with DAPA-HF (all-cause death HR 0.83, P=0.017 in HFrEF) and even with DELIVER's directional trend. HFpEF carries a meaningful annual mortality (~5–8%/year in trial populations), yet no pharmacotherapy has demonstrated mortality benefit. The Class I, Level A recommendation for SGLT2i rests entirely on composite HF hospitalisation reduction in a population where mortality remains unaddressed. (sources/empagliflozin-hfpef-nejm-2021, rating: very high)
- EMPEROR-Preserved: high discontinuation rate (23%) may bias toward null for hard outcomes: Nearly 1-in-4 patients stopped trial medication (similar in both groups), limiting the ability to detect mortality effects and potentially diluting the true composite benefit. This is higher than DAPA-HF (10.5%/10.9%) and DELIVER, and may partly explain why the primary benefit was driven by hospitalisation rather than mortality. (sources/empagliflozin-hfpef-nejm-2021, rating: very high)
- NT-proBNP thresholds not mandated in recommendation: Trial entry required elevated natriuretic peptides; the 2023 task force chose not to specify thresholds in the recommendation text, creating uncertainty about treating HFpEF with low natriuretic peptides. (sources/HF-update-ESC-2023, rating: very high)
- Finerenone (FINEARTS-HF) and SGLT2i: both reduce HF hospitalizations but neither reduces mortality in HFpEF — cumulative pharmacotherapy failure for mortality reduction: As of 2024, every pharmacotherapy trial in HFpEF (MRA, SGLT2i, ARNI, ARB, RAAS inhibition, PDE5 inhibitor, sGC stimulator) has failed to demonstrate a significant mortality benefit. FINEARTS-HF joins this pattern — CV death HR 0.93 (NS); all-cause death HR 0.93 (NS). The inability to reduce mortality despite meaningful HF hospitalization reduction suggests HFpEF mortality is driven by mechanisms (cancer, non-CV death, frailty) not targeted by these drugs, or that the disease is too heterogeneous for any single agent to show mortality benefit. (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high)
- Finerenone vs spironolactone in HFpEF — not a direct comparison: TOPCAT (spironolactone, HR 0.89, P=0.14) and FINEARTS-HF (finerenone, rate ratio 0.84, P=0.007) differ in: drug pharmacology, endpoint analysis method (time-to-first vs total events), background therapy (no SGLT2i in TOPCAT era vs 13.6% in FINEARTS-HF), follow-up duration, and critically — TOPCAT had severe data integrity problems in Russia/Georgia. It cannot be concluded that finerenone is superior to spironolactone; the apparent divergence in significance may largely reflect trial design and data integrity differences. (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high; sources/spironolactone-hfpef-topcat-nejm-2014 — high)
- Intentional weight loss refutes the obesity paradox in HFpEF: Observational data had suggested weight loss was associated with worse HF prognosis (the "obesity paradox"), discouraging weight-loss strategies in HF. STEP-HFpEF demonstrates the opposite — that intentional pharmacologic weight loss (−13.3%) produces large improvements in symptoms, functional capacity, and fewer cardiac events in obesity-HFpEF. The reconciliation is that prior observational data captured unintentional weight loss from cardiac cachexia; intentional weight loss via pharmacotherapy is a fundamentally different phenomenon. (sources/semaglutide-stephfpef-nejm-2023, rating: very high)
- Semaglutide KCCQ improvement 4–15× larger than all prior HFpEF pharmacotherapy — mechanism unclear: The +7.8-point KCCQ-CSS difference far exceeds prior HFpEF trials (SGLT2i/ARNI/spironolactone: 0.5–2.3 points). This cannot be attributed to weight loss alone — the NT-proBNP fall despite weight loss and the 43.5% CRP reduction implicate direct hemodynamic and anti-inflammatory drug effects. The relative contributions of weight loss vs. direct GLP-1 signaling remain unresolved and cannot be disentangled without a trial design that isolates these mechanisms (e.g., matched weight loss control arm). (sources/semaglutide-stephfpef-nejm-2023, rating: very high)
- Tirzepatide (SUMMIT): numerically higher all-cause and CV deaths despite reduced HF events — divergent signals within the same trial: The composite HF outcome was significantly reduced (HR 0.62), yet all-cause deaths were numerically higher (19 vs 15; HR 1.25) and CV/undetermined deaths numerically higher (10 vs 5; HR 1.58), both non-significant. Authors propose HFpEF CV deaths usually do not reflect HF progression (11 of 15 total CV deaths not preceded by worsening HF), and prior GLP-1 RA outcome trials in obesity/T2DM show mortality reduction over longer follow-up. However, this divergence — fewer HF events but no mortality reduction — raises an unresolved question: does tirzepatide defer HF events without altering the underlying mortality trajectory in HFpEF? (sources/tirzepatide-hfpef-summit-nejm-2025, rating: very high)
- SUMMIT primary endpoint revision and NP threshold question: SUMMIT amended endpoints ~1 year before trial completion following FDA discussion, and notably did not require elevated NT-proBNP for enrollment (median NP <200 pg/mL). This challenges the premise that elevated natriuretic peptides should be required to initiate GLP-1 RA or dual GIP/GLP-1 RA therapy in obesity-HFpEF — subgroup analysis confirmed benefit even at NP <200 pg/mL. However, this also means the trial enrolled patients who may not meet guideline HFpEF definitions requiring elevated NP, limiting regulatory applicability. (sources/tirzepatide-hfpef-summit-nejm-2025, rating: very high)
- Finerenone kidney composite numerically worse in HFpEF (HR 1.33) vs nephroprotective in CKD-T2DM: FIDELIO-DKD and FIGARO-DKD established finerenone as nephroprotective in CKD+T2DM patients with significant albuminuria. FINEARTS-HF enrolled a low-albuminuria population with few kidney events — this patient profile may explain the absence (and numerical reversal) of a kidney benefit, and cautions against assuming nephroprotection from finerenone in HFpEF without significant CKD. (sources/finerenone-hfpef-fineartshf-nejm-2024 — very high)
- Titin isoform switch direction in HFpEF is inconsistent: Some studies show increased N2BA:N2B ratio (lower stiffness), others do not — the role of isoform switching as compensatory vs. pathological in HFpEF remains unresolved. (sources/TTN-CVResearch-2022, rating: high)
- cGMP-PKG pathway as therapeutic target has failed in clinical trials: Despite strong pre-clinical mechanistic rationale (RELAX, VITALITY, SOCRATES all negative), suggesting the titin phosphorylation model may be insufficient or not translatable in humans. (sources/TTN-CVResearch-2022, rating: high)
- COPD diagnosis accuracy in HFpEF — systematic over/under-diagnosis: HF causes pulmonary oedema, bronchial mucosal oedema, and reduced lung CO diffusion that can mimic COPD on spirometry; conversely, effective HF treatment can normalize spirometry. This confounds both COPD diagnosis and the prognostic data from studies relying on clinically-diagnosed COPD (most included in the 2025 meta-analysis). The true COPD prevalence and its independent prognostic weight in HFpEF may differ from estimates based on clinical diagnosis alone. (sources/copd-hfpef-eschf-2025, rating: high)
Connections
- Related to concepts/Atrial-Cardiomyopathy — mechanical atrial dysfunction independent predictor in HFpEF; disproportionate LA myopathy phenotype
- Related to concepts/Atrial-Failure — atrial failure and HFpEF phenotypes overlap
- Related to entities/Heart-Failure
- Related to concepts/LV-Diastolic-Function — echo-based HFpEF diagnosis algorithm
- Related to entities/Atrial-Fibrillation — elevated NT-proBNP thresholds differ in AF patients
- Related to entities/Fabry-Disease — AFD as genetic cause of HFpEF
- Related to concepts/Fabry-Cardiomyopathy
- Related to entities/ATTR-Amyloidosis — infiltrative cause of HFpEF
- Related to concepts/Titin-PTMs
- Related to concepts/Titin-Isoform-Switch
- Related to sources/HF-ESC-2021
- Related to sources/HF-update-ESC-2023
- Related to sources/HF-AHA-2022
- Related to sources/echo-hfpef-ase-2025
- Related to sources/TTN-CVResearch-2022
- Related to sources/fabry-ehj-2024
- Related to entities/Obesity — obesity-HFpEF distinct phenotype
- Related to concepts/Visceral-Adiposity — epicardial fat and pericardial restraint in obesity-HFpEF
- Related to concepts/Obesity-Paradox — less consistent in HFpEF than HFrEF
- Related to sources/obesity-cv-aha-2021
- Related to sources/atrial-cmp-esc-2025
- Related to sources/ch-aha-2026
- Related to concepts/Clonal-Hematopoiesis — TET2-CH 2.4× enriched in HFpEF; NLRP3/IL-1β mechanism
- Related to entities/Sacubitril-Valsartan — ARNI; PARAGON-HF trial primary evidence; COR 2b in AHA 2022
- Related to sources/dapagliflozin-deliver-nejm-2022 — DELIVER RCT; primary evidence for SGLT2i in HFpEF/HFmrEF
- Related to sources/empagliflozin-hfpef-nejm-2021 — EMPEROR-Preserved RCT; first large positive HFpEF pharmacotherapy trial
- Related to entities/Finerenone — nonsteroidal MRA; FINEARTS-HF trial
- Related to sources/finerenone-hfpef-fineartshf-nejm-2024 — FINEARTS-HF RCT; first MRA with positive primary endpoint in HFpEF
- Related to entities/Semaglutide — GLP-1 RA; STEP-HFpEF; largest symptom improvement of any HFpEF pharmacotherapy trial
- Related to sources/semaglutide-stephfpef-nejm-2023 — STEP-HFpEF RCT; first obesity-targeting pharmacotherapy in HFpEF
- Related to entities/Tirzepatide — dual GIP/GLP-1 RA; SUMMIT; first hard composite endpoint benefit in obesity-HFpEF
- Related to sources/tirzepatide-hfpef-summit-nejm-2025 — SUMMIT RCT; HR 0.62 composite CV death or worsening HF
- Related to entities/COPD — independent prognostic risk factor in HFpEF; prevalence 14–34%; shared microvascular inflammation pathway; β-blockers contraindicated in HFpEF+COPD
- Related to concepts/HF-COPD-Comorbidity — bidirectional pathophysiology; diagnostic challenges; treatment interactions
- Related to concepts/Cardiopulmonary-Exercise-Testing — CPET in HFpEF diagnostic workup; VE intercept as COPD identifier
- Related to sources/copd-hfpef-eschf-2025 — systematic review/meta-analysis (n=18,602); COPD increases hospitalization RR 1.66, mortality RR 1.62, post-discharge mortality RR 2.57
- Related to sources/hf-copd-hfreview-2025 — 2025 review; β-blockers to avoid in HFpEF+COPD; NP diagnostic limitations; CPET VE intercept
Sources
- sources/HF-AHA-2022
- sources/HF-ESC-2021
- sources/HF-update-ESC-2023
- sources/dapagliflozin-deliver-nejm-2022
- sources/TTN-CVResearch-2022
- sources/atrial-cmp-esc-2025
- sources/ch-aha-2026
- sources/echo-hfpef-ase-2025
- sources/fabry-ehj-2024
- sources/obesity-cv-aha-2021
- sources/arni-paragon-hf-nejm-2019
- sources/empagliflozin-hfpef-nejm-2021
- sources/spironolactone-hfpef-topcat-nejm-2014
- sources/finerenone-hfpef-fineartshf-nejm-2024
- sources/semaglutide-stephfpef-nejm-2023
- sources/tirzepatide-hfpef-summit-nejm-2025
- sources/copd-hfpef-eschf-2025
- sources/hf-copd-hfreview-2025