Intra-Aortic Balloon Pump (IABP)
Definition
The intra-aortic balloon pump (IABP) is the most widely used temporary mechanical circulatory support device. A balloon mounted on a catheter in the descending thoracic aorta inflates in diastole (augmenting coronary and systemic perfusion) and deflates in systole (reducing LV afterload) — the principle of "counterpulsation."
Key Concepts
History
- Counterpulsation principle described experimentally by Kantrowitz brothers in 1952
- Moulopoulos et al developed the intra-aortic balloon device in 1962
- First clinical use by Kantrowitz et al (1968): 2 CS patients; hemodynamic improvement in both; 1 survived to discharge
- Percutaneous insertion described by Bregman et al (1980) — now the standard technique sources/iabp-ajc-2006 (medium)
Device Operation
- Double-lumen 8–9.5 Fr catheter; 25–50 mL balloon; helium gas (low density = rapid transmission)
- Balloon sizing by patient height: <5 ft → 25 mL; 5–5'4" → 34 mL; 5'4"–6' → 40 mL; >6' → 50 mL; maximum expanded diameter ≤80–90% of descending thoracic aorta
- Tip positioned 2–3 cm distal to left subclavian artery origin (level of carina); confirmed fluoroscopically
- Inner lumen: continuous arterial pressure monitoring; outer lumen: helium delivery
- Cycling: 1:1 (maximum support), 1:2 (initial/assessment mode), 1:4/1:8 (weaning)
- Non-functioning balloon must be removed within 30 minutes (thrombosis risk) sources/iabp-ajc-2006 (medium)
Triggering
- ECG trigger: R wave peak → deflation (LV systole); T wave midpoint → inflation (LV diastole); unreliable in AF or poor ECG quality
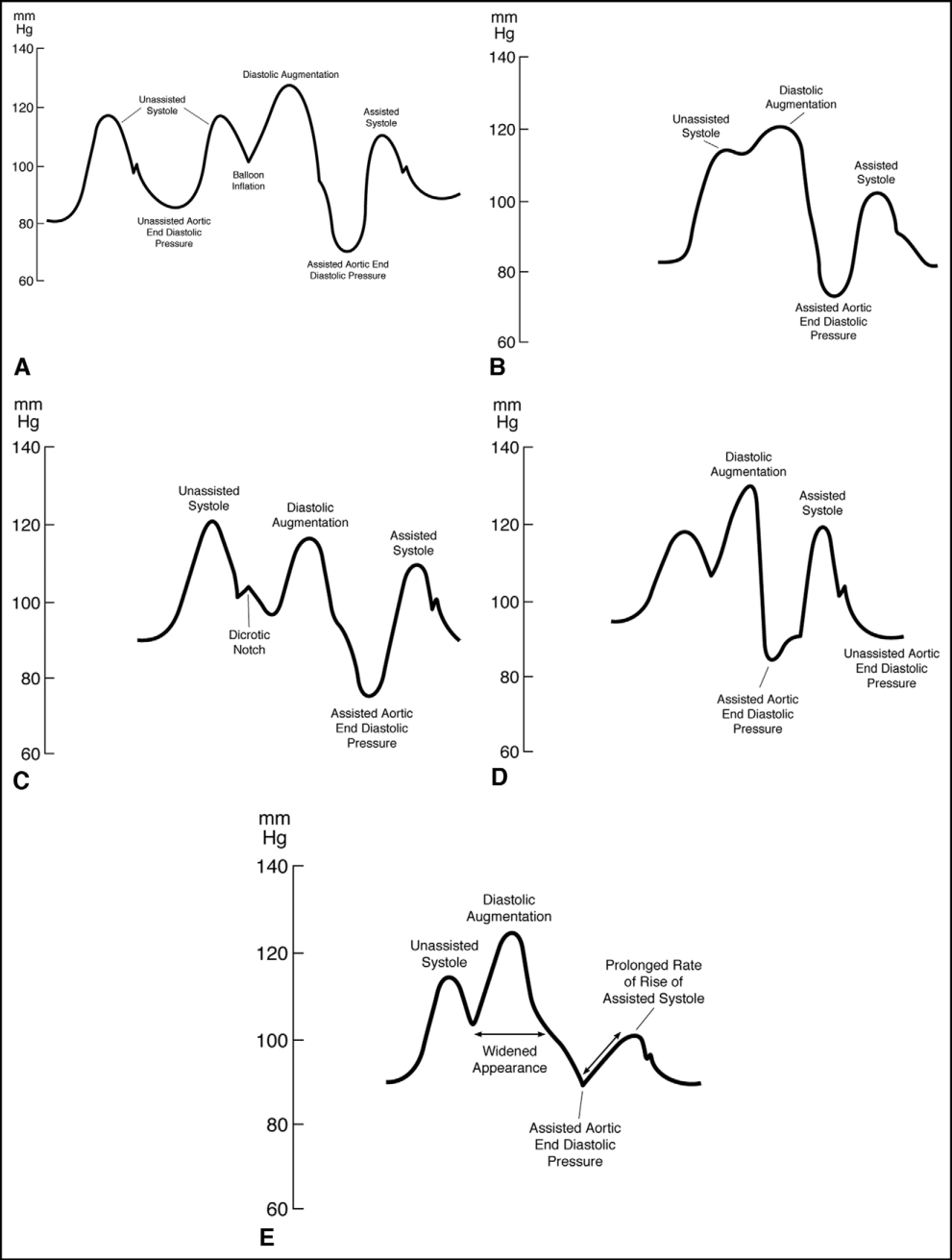
- Arterial pressure waveform trigger: inflate at dicrotic notch (aortic valve closure); deflate just before systolic upstroke (before aortic valve opening)
- Waveform must be assessed daily by trained personnel sources/iabp-ajc-2006 (medium)
Timing Errors and Their Consequences
| Timing Error | Hemodynamic Consequence |
|---|---|
| Early inflation (before aortic valve closure) | LV ejects against inflated balloon → ↑ afterload, ↑ O2 demand, worsening systolic function |
| Late inflation (well after diastole onset) | Reduced diastolic pressure augmentation → less coronary/systemic perfusion benefit |
| Early deflation (before diastole ends) | Shortened augmentation; transient pressure drop → retrograde flow from carotid/coronary arteries → cerebral/myocardial ischemia risk |
| Late deflation (after diastole ends) | Balloon still inflated at systole → same as early inflation: ↑ afterload, ↑ O2 demand |
Optimal: peak diastolic augmentation > unassisted systolic pressure; assisted end-diastolic and assisted systolic pressures both < unassisted values sources/iabp-ajc-2006 (medium)
Hemodynamic Effects
LV performance:
- Effect magnitude depends on balloon volume, heart rate, and aortic compliance
- Higher HR → shorter diastolic filling time → less augmentation per beat
- Higher aortic compliance (lower SVR) → attenuated augmentation
- Hypotensive patients: net MAP increase (diastolic augmentation exceeds systolic decrease)
- Normotensive patients: little/no MAP change (circulatory autoregulation maintains pressure)
- Cardiogenic shock/severe HF: systolic unloading → ↓ LV wall tension and O2 demand → secondary ↓ preload (LA pressure/LVEDP) → ↑ SV and CO sources/iabp-ajc-2006 (medium)
Coronary blood flow:
- Theoretical: diastolic pressure augmentation should increase coronary flow (most coronary flow occurs in diastole)
- Evidence conflicting — studies show increase, no change, or decrease depending on patient hemodynamics, species, and measurement method
- Benefit occurs in patients with impaired autoregulation (profound hypotension beyond the 45–125 mmHg autoregulatory range)
- Fixed severe stenosis (>90%): diastolic pressure increase NOT transmitted to poststenotic segment — no poststenotic coronary flow benefit sources/iabp-ajc-2006 (medium)
Clinical Indications and Evidence
Cardiogenic shock (~20% of all IABP insertions):
- SHOCK Trial Registry: IABP + thrombolysis 47% vs thrombolysis alone 63% vs neither 77% mortality — significant confounding by higher revascularization rates in IABP group
- NRMI-2 (n=23,180 AMI-CS): IABP + thrombolysis 49% vs 67% without IABP (P<0.001; benefit); IABP + primary PCI 45% vs 47% (NS — no benefit) — foreshadows IABP-SHOCK II sources/iabp-ajc-2006 (medium)
- IABP-SHOCK II (2013): no 30-day mortality benefit; no improvement at 6-year follow-up in AMI-CS undergoing PCI sources/mcs-jic-2023 (high)
- ESC 2014: downgraded from Class I → Class III (not recommended) in ACS-CS sources/mcs-jic-2023 (high)
- JCS guidelines: Class I for mechanical complications of AMI; Class IIa for refractory ischemia post-reperfusion; Class III for routine CS use sources/mcs-jic-2023 (high)
- Hemodynamic improvement is common but does NOT reliably translate to mortality benefit without revascularization
VSR / papillary muscle rupture with acute MR (~5% of IABP use):
- Small observational series: hemodynamic improvement, reduced intracardiac shunting, improved PAWP and systemic pressure sources/iabp-ajc-2006 (medium)
Intractable ventricular arrhythmias:
- Fotopoulos et al (n=21 medically refractory VA): 18/21 showed arrhythmia reduction or abolition — mechanistic basis: improved coronary perfusion reducing ischemic arrhythmia trigger sources/iabp-ajc-2006 (medium)
Post-MI / unstable angina refractory to medical therapy (~12% of IABP use):
- Observational: symptomatic and ECG improvement; no RCT data sources/iabp-ajc-2006 (medium)
Refractory HF: bridge to cardiac transplantation only (temporary) sources/iabp-ajc-2006 (medium)
High-risk PCI: no randomized data supporting prophylactic use; routine post-primary-PCI IABP NOT indicated (RCT n=437: no difference in death, reinfarction, or reocclusion) sources/iabp-ajc-2006 (medium)
High-risk CABG (with ongoing ischemia/decompensated HF/hemodynamic instability):
- Preoperative IABP associated with lower mortality in observational series and one small RCT (n=52; 6% vs 25%; P<0.05)
- NOT recommended for left main CAD without ischemia, or poor LV function without overt HF sources/iabp-ajc-2006 (medium)
Contraindications
- Absolute: aortic regurgitation (worsens regurgitation); aortic dissection (false lumen placement risk); sizable abdominal aortic aneurysm (rupture risk)
- Relative/Procedural: severe peripheral vascular disease uncorrectable by angioplasty/surgery; bilateral femoral-popliteal bypass grafts; uncontrolled septicemia; bleeding diathesis
- Aortobifemoral bypass grafts: generally acceptable for percutaneous femoral IABP sources/iabp-ajc-2006 (medium)
Complications
Benchmark Registry (n=16,909; largest multinational registry):
- Any complication: 7%
- Major complications: 2.6%
- Limb-threatening ischemia: 0.9%
- Major bleeding: 0.8%
- Limb amputation: 0.1%
- IABP-related death: 0.05% (usually aortic dissection/rupture)
Predictors of major complications (multivariate):
- Age >75 years
- Peripheral vascular disease
- Diabetes mellitus
- Female gender
- Small body surface area (<1.65 m²) sources/iabp-ajc-2006 (medium)
Hematologic: hemoglobin falls ~2.3 g/dL (hemolysis + access site bleeding); thrombocytopenia from mechanical platelet destruction ± heparin; monitor daily CBC and creatinine
Anticoagulation: heparin aPTT target 50–70 seconds standard; one RCT (n=153) showed no difference in limb ischemia with vs without heparin — benefit of routine heparin remains unproven sources/iabp-ajc-2006 (medium)
Note: Benchmark Registry complication rates substantially lower than later systematic reviews (Kapur et al.: major bleeding 12.9%, limb ischemia 1.5%, stroke 3.1%) — reflecting registry under-reporting and center selection bias sources/mcs-jic-2023 (high)
Contradictions / Open Questions
- Coronary flow augmentation: mechanistically logical but evidence conflicting — does not reliably increase flow distal to severe fixed stenoses; clinical relevance of coronary augmentation in the PCI era uncertain
- Anticoagulation necessity: standard heparin practice is not RCT-validated; single RCT showed no limb ischemia difference — practice varies
- Complication rate discrepancy: Benchmark Registry (0.9% limb-threatening ischemia) vs Kapur systematic review (1.5% limb ischemia overall) — registry data likely underestimates real-world complication burden
- IABP in primary PCI era: NRMI-2 (2001) showed no benefit with IABP + primary PCI; IABP-SHOCK II (2013) confirmed null result — yet IABP remains widely used for mechanical complications of MI where evidence is observational only
- JCS vs ESC vs ACC guideline discordance: JCS retains Class IIa for refractory post-reperfusion ischemia; ESC Class III; ACC 2025 does not recommend routine IABP — no RCT in mechanical MI complications exists
Connections
- Related to concepts/Temporary-Mechanical-Circulatory-Support
- Related to concepts/Cardiogenic-Shock
- Related to concepts/ECPELLA
- Related to concepts/SCAI-Shock-Classification