LBBB Criteria
Definition
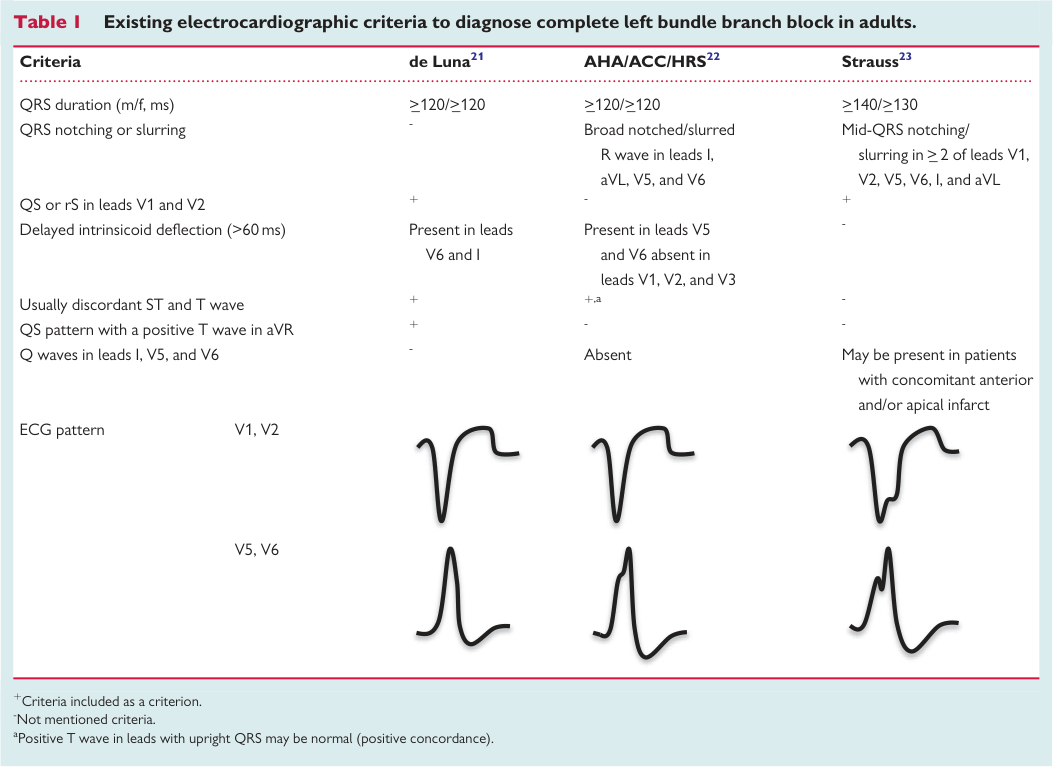
Left bundle branch block (LBBB) is a conduction disturbance caused by failure of conduction along the anterior, mid, and posterior left fascicles of the His-Purkinje system. The diagnostic criteria remain contested — conventional AHA criteria (QRS ≥120 ms) have high sensitivity but low specificity, while Strauss' strict criteria (QRS ≥140/130 ms men/women + mid-QRS notching/slurring) better identify "true" LBBB with intact septal block, which is the morphology that predicts CRT response.
Key Concepts
Conventional AHA/ACCF/HRS Criteria (Surawicz 2009)
- QRS ≥120 ms (adults ≥18 yr); ≥100 ms (4–17 yr); ≥90 ms (<4 yr)
- Wide notched or slurred R wave in leads I, aVL, V5–V6
- Absent q waves in leads I, V5–V6
- R-wave peak time (VAT) >60 ms in V5–V6; normal in V1–V3
- Discordant ST segment and T waves (appropriate discordance)
- These criteria were used in COMPANION, CARE-HF, and RAFT trials
- (sources/ecg-bbb-aha-2009, high) (sources/lbbb-evg-ane-2019, high)
Strauss' Strict Criteria (Strauss 2011)
- QRS ≥140 ms (men) or ≥130 ms (women) >18 yr
- QS or rS in V1 and V2
- Mid-QRS notching or slurring in ≥2 contiguous leads of: V1, V2, V5, V6, I, aVL
- Notching/slurring must appear after the initial 40 ms of the QRS
- Increases specificity for true LBBB, especially in presence of LVH/dilatation or incomplete LBBB
- (sources/lbbb-evg-ane-2019, high)
Why Strict Criteria Matter for CRT
- ~1/3 of patients diagnosed with LBBB by conventional criteria may not have true LBBB — likely have LVH + LAFB combination
- ~30% of CRT patients are non-responders, partially attributed to false LBBB selection
- Strict LBBB criteria better predict echocardiographic CRT response and reduced HF hospitalization (Mascioli 2012, Garcia-Seara 2018)
- However: Bertaglia 2017 showed stricter criteria did NOT improve CRT response vs AHA definition — controversy unresolved
- (sources/lbbb-evg-ane-2019, high)
Additional ECG Features of True LBBB
- Initial r wave ≥1 mm in V1: suggests intact left-to-right septal activation; found in ~28% of conventionally-defined LBBB; proposed exclusion criterion for CLBBB; also identifies patients at low risk of complete heart block during right heart catheterization
- QRS transition zone delayed to V5 or beyond: novel SCD risk marker (Aro 2014)
- Prolonged R-wave peak time (VAT) ≥60 ms in I, V5–V6
- (sources/lbbb-evg-ane-2019, high)
Concordant vs Discordant LBBB
| Feature | Concordant LBBB | Discordant LBBB |
|---|---|---|
| Frequency | ~28–32% | ~68–70% |
| Age | Relatively younger | Relatively older |
| LVEF | Higher (mean ~51%) | Lower (mean ~36%) |
| LV end-diastolic diameter | Smaller | Larger |
| QRSd | Shorter (mean ~151 ms) | Longer (mean ~160 ms) |
| BNP | Lower | Higher |
| Coronary artery disease | Less | More frequent |
| Prognosis | Better | Worse |
| CRT benefit | Less | Greater |
| VT/VF | Less frequent | More frequent (NS) |
- Concordant LBBB (cLBBB): T-wave orientation concordant with QRS — positive/diphasic T wave in ≥2 of leads I, V5, V6
- Discordant LBBB (dLBBB): ST segments and T waves opposite to main QRS deflection — observed in ~70% of uncomplicated LBBB; also called "appropriate discordance"
- Discordant LBBB associated with more severe CAD and worse prognosis even with CRT-D (Padeletti 2018)
- (sources/lbbb-evg-ane-2019, high)
QRS Area (VCG-Derived) — Superior CRT Predictor
- QRS area from VCG is a stronger predictor of CRT response than QRS duration and conventional LBBB morphology (van Deursen 2015a,b; Rad 2016) sources/vcg-fronphysiol-2022 (medium)
- Rad 2016: 51 VCGs derived by Kors regression method — QRS area is a non-invasive alternative to intracardiac measurement identifying delayed LV lateral wall activation better than QRS duration or LBBB morphology
- Combined CMR scar parameters + QRS area (Kors VCG): highest CRT response prediction (Nguyên 2018): patients with low focal scar + high QRS area have highest CRT response rate
- Reducing QRS area (QRS area improvement post-CRT) predicts acute hemodynamic response (Okafor 2020)
- New vs old LBBB distinction: QRS/T vector magnitude ratio and deepest-S/largest-T ratio (IDT-derived VCG) allow 100% sensitivity, 96–68% specificity (Shvilkin 2010) — useful in chest pain + LBBB presentation
- (sources/vcg-fronphysiol-2022, medium)
Vectorcardiographic (VCG) Criteria for True CLBBB (Horizontal Plane)
- Narrow, elongated QRS loop; usually figure-of-8 rotation
- QRS loop duration ≥130 ms (women) or ≥140 ms (men)
- Main body inscribed posteriorly and to the left (−90° to −40°)
- Maximal QRS vector in left posterior quadrant (−40° to −80°), magnitude >2 mV
- Main QRS loop rotation: clockwise (counterclockwise suggests parietal CLBBB, lateral infarction, or LVH)
- Middle + end conduction delay: pathognomonic of true LBBB — absence of this finding in a QRS loop differentiates pseudo-LBBB from true LBBB
- ST/T-wave vector directed rightward and anteriorly; QRS/ST-T angle ≥90° (discordant) or <90° (concordant)
- (sources/lbbb-evg-ane-2019, high)
Gender Differences in LBBB
- Women exhibit LBBB pattern at shorter QRSd and have more frequent mechanical dyssynchrony at shorter QRSd than men
- Explains better CRT response rates in women at shorter QRSd (De Pooter 2018)
- Strauss criteria use gender-specific thresholds (≥140 ms men / ≥130 ms women)
- (sources/lbbb-evg-ane-2019, high)
TAVR-Induced LBBB
- Incidence 7–83% depending on device; systematic review: 14.0% for Sapien (4.0–30.2%) vs 45.2% for CoreValve (22.0–65.0%)
- Mechanism: proximity of AV node and left bundle branch to aortic valve; mechanical interaction of valve frame with conduction system structures
- Predictors: device geometry, baseline QRS duration, pre-procedural RBBB, male gender, prior MI, prior CABG, depth of implantation
- Dutch registry: All-cause mortality 37.8% vs 24.0% (P=0.002) in TAVR-LBBB vs no-LBBB; iatrogenic LBBB was the strongest independent predictor of mortality
- PARTNER trial subanalysis: TAVR-induced LBBB NOT associated with 1-year all-cause mortality, stroke, or MI — only associated with pacemaker implantation; conflicting data explained by patient selection differences (exclusion of pre-existing conduction abnormalities) and timing of LBBB determination (transient vs persistent)
- Post-TAVR LBBB associated with decrease in LVEF; persistent LBBB after surgical AVR much less common (<2%)
- (sources/lbbb-europace-2017, high)
Pathophysiology of Mechanical Dyssynchrony in LBBB
- Block in Purkinje system → cell-to-cell myocardial conduction → RV free wall + IVS contract before LV lateral wall
- Septal flash (SF): Early rapid leftward IVS motion driven by RV free wall contraction (NOT active IVS contraction per computer simulation); amplitude modulated by diastolic ventricular pressures
- SF ≠ septal systolic rebound stretch: SF is M-mode early systolic IVS motion; septal systolic rebound stretch (measured by strain echo) depends on late LV lateral wall contraction forces — distinct mechanisms, not interchangeable
- Apical rocking: Back-and-forth apex motion — initially toward septum (early IVS contraction), then lateral (late LV lateral wall contraction); highly specific for LBBB-induced dyssynchrony
- Lateral wall hypertrophy from disproportionate ejection work; reduced septal perfusion and relative lateral hyperperfusion
- Long-term consequences: LV dilation, asymmetric hypertrophy, decreased pump function, functional MR (annular dilation + dyssynchronous papillary muscles), pro-arrhythmic state
- (sources/lbbb-europace-2017, high)
Echocardiographic CRT Predictors
- SF + apical rocking before CRT = better CRT outcomes and long-term survival; correction of both by CRT = LV reverse remodeling
- 1/3 of LBBB patients selected for CRT do not show typical speckle-tracking contraction pattern; ECG-mechanics mismatch independently associated with adverse outcomes
- Apical rocking (26%) and SF (20%) observed in CRT patients without typical LBBB ECG morphology — most responded to CRT — imaging can identify CRT responders independent of ECG morphology
- Systolic stretch index (SSI) >9.7%: Sum of posterior-lateral pre-ejection prestretch + septal systolic rebound stretch from 2D speckle-tracking radial strain (mid-LV short-axis view); independently predicts favorable CRT outcomes even at intermediate QRS duration (120–149ms) where ECG criteria alone are insufficient
- LV pressure-strain loop area (myocardial work): Septum in LBBB + chronic HF performs net negative work (systolic lengthening); after CRT, proportion of positive septal work increases dramatically
- (sources/lbbb-europace-2017, high)
Prognosis of LBBB
- LBBB associated with increased cardiovascular mortality, SCD, and heart failure vs normal conduction and vs RBBB
- 3983-subject, 29-year longitudinal study: SCD often the first manifestation; patients developing LBBB <45 years without risk factors had better prognosis than those ≥50 years with risk factors
- Prolonged QRS ≥110ms (any morphology) predicts all-cause/cardiac mortality and sudden arrhythmic death; LBBB morphology alone predicts only sudden arrhythmic death
- In HF with LVEF ≤39%: LBBB and other IVCDs (including RBBB) are equally strong independent predictors of mortality in all age groups
- New-onset LBBB should be considered pathological; may indicate acute MI (concordant LBBB = Sgarbossa criteria)
- Isolated LBBB in otherwise normal heart: causes mechanical asynchrony, LV EF reduction, and redistribution of circumferential shortening — can initiate LV remodeling (Vernooy 2005)
- LBBB may be a sign of progressive degenerative disease affecting both the conduction system and myocardium (Eriksson 2005, 28-year follow-up)
- HV interval ≥70 ms (especially ≥100 ms) predicts progression to spontaneous AV block
- (sources/lbbb-evg-ane-2019, high); (sources/lbbb-europace-2017, high)
Contradictions / Open Questions
- Strauss vs conventional criteria for CRT selection: Strict Strauss criteria better identify true LBBB (mechanistically), but Bertaglia 2017 found no improvement in CRT response using strict criteria vs AHA definition — the criteria paradox remains unresolved
- TAVR-LBBB prognosis: Dutch registry shows TAVR-LBBB as strongest independent predictor of mortality (37.8% vs 24.0%; P=0.002); PARTNER trial subanalysis shows no 1-year mortality difference — conflicting data explained by differences in patient selection (exclusion of pre-existing conduction abnormalities), pacemaker inclusion, and transient vs persistent LBBB classification (sources/lbbb-europace-2017, high)
- ECG vs imaging for CRT candidate selection: 1/3 of LBBB patients lack typical echocardiographic dyssynchrony pattern on speckle tracking; yet apical rocking/SF are seen in 20–26% of CRT patients without LBBB ECG morphology and most respond — suggests ECG criteria misclassify in both directions (sources/lbbb-europace-2017, high)
- Systolic stretch index clinical integration: SSI >9.7% predicts CRT response at intermediate QRS (120–149ms) where guidelines are equivocal, but this cut-off requires prospective validation in large multicenter cohorts before routine use (sources/lbbb-europace-2017, high)
- Gender-specific QRS thresholds: Strauss uses different thresholds for men/women; current AHA/ESC guidelines do not incorporate gender-specific thresholds; may contribute to underrepresentation of women in CRT benefit analyses
- VCG availability: VCG identifies true LBBB more definitively but is not routinely available in most clinical settings, limiting its practical utility
- Concordant LBBB and CRT benefit: While discordant LBBB has greater CRT benefit in registry data, this distinction has not been incorporated into formal guideline-based CRT selection criteria
- Global vs single-lead QRS measurement: AHA 2009 global measurement standard yields systematically longer QRS durations than the single-lead measurements used in CRT trials establishing the ≥150 ms threshold — an unresolved calibration discrepancy (see concepts/ECG-Conduction-Disturbances)
Connections
- Related to concepts/ECG-Conduction-Disturbances — foundational AHA 2009 LBBB criteria and general conduction disturbance classification
- Related to concepts/Cardiac-Resynchronization-Therapy — LBBB morphology is the primary ECG predictor of CRT response; strict vs conventional criteria debate
- Related to concepts/Sgarbossa-Criteria — concordant LBBB (negative concordance) as marker of acute coronary occlusion
- Related to concepts/Atrioventricular-Block — HV interval in BBB predicts AV block progression
- Related to entities/Vectorcardiography — VCG as definitive tool for true vs pseudo-LBBB; QRS area as CRT predictor; transformation methods (Kors vs IDT); VCG superiority in LQTS, MI, atrial enlargement
Sources
- sources/ecg-bbb-aha-2009 — AHA/ACCF/HRS 2009 conventional LBBB criteria
- sources/lbbb-evg-ane-2019 — Strauss strict criteria, concordant/discordant distinction, VCG criteria, CRT non-responder problem
- sources/vcg-fronphysiol-2022 — QRS area from VCG as stronger CRT predictor; new vs old LBBB VCG discrimination
- sources/lbbb-europace-2017 — TAVR-induced LBBB (incidence, prognosis); pathophysiology (SF, apical rocking, lateral hypertrophy); echocardiographic CRT predictors (SSI >9.7%, myocardial work); stress testing meta-analysis; Sgarbossa performance data