Temporary Mechanical Circulatory Support
Definition
Temporary mechanical circulatory support (tMCS) devices augment cardiac output, promote ventricular unloading, and restore systemic perfusion in cardiogenic shock. They serve as a bridge to myocardial recovery, advanced therapies (durable LVAD, heart transplant), or palliation. Common devices include intra-aortic balloon pumps (IABP), microaxial flow pumps (Impella), and venoarterial extracorporeal membrane oxygenation (VA-ECMO).
Key Concepts
Mechanistic Goals
- Promote ventricular unloading (reduce myocardial work and oxygen consumption)
- Restore systemic perfusion and cardiac index
- Allow de-escalation of vasoactive medications that may cause myocardial damage at high doses/prolonged duration
- Bridge to: myocardial recovery | durable LVAD | heart transplant | palliative care sources/cardiogenic-shock-acc-2025 (very high)
MODS Primacy and Timing — Why Hemodynamics Alone Are Insufficient
- MODS severity (APACHE II/SAPS II scores) and SIRS biomarkers (IL-6, RAGE) predict CS mortality more accurately than hemodynamic indices (CI, BNP) sources/mcs-ehj-2014 (medium)
- Cardiac index alone is unrelated to survival beyond the first 24 h of AMI-CS; BNP also unrelated to prognosis in the first 96 h sources/mcs-ehj-2014 (medium)
- Cardiac power output/index is the single strongest hemodynamic correlate of mortality in CS (SHOCK trial registry) — superior to CI or MAP in isolation sources/mcs-ehj-2014 (medium)
- Once MODS is established, increasing CO with MCS may not reverse end-organ failure — haemodynamic improvement ≠ mortality benefit
- Three prerequisites for MCS to translate into survival: (1) early timing before MODS established; (2) adequate CI restoration; (3) prevention of device-related complications sources/mcs-ehj-2014 (medium)
- MCS should NOT be last-resort therapy; early initiation minimizes high-dose catecholamine microvascular toxicity and prevents MODS progression sources/mcs-ehj-2014 (medium)
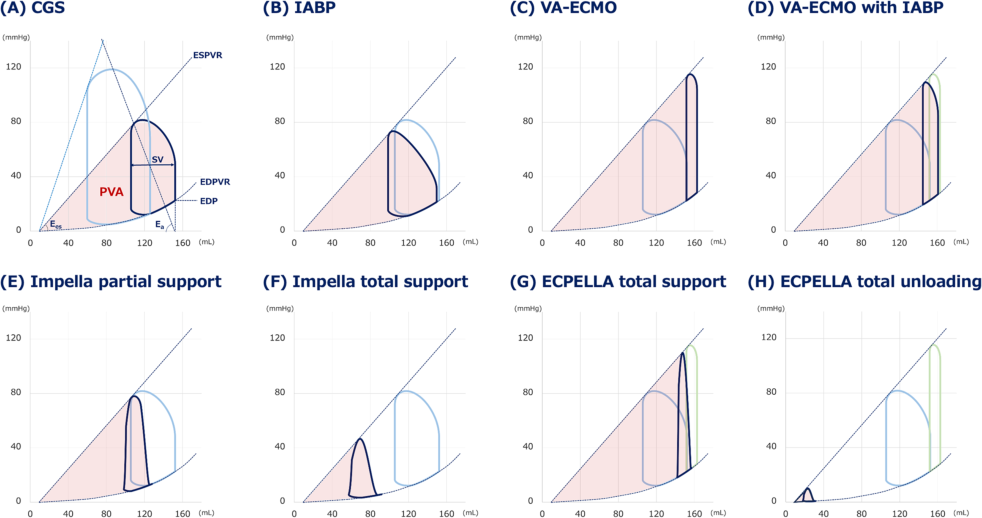
PV Loop Framework — Device Hemodynamics
The pressure-volume (PV) loop quantifies LV mechanical work; PVA (pressure-volume area) is linearly related to myocardial O2 consumption sources/mcs-jic-2023 (high):
- IABP: rapid deflation in systole reduces end-systolic pressure → modest SV increase; no direct diastolic LV effect; augments coronary perfusion via diastolic inflation
- VA-ECMO: retrograde aortic flow increases LV afterload → PV loop shifts rightward, PVA enlarges (worsens myocardial O2 demand); adding IABP to VA-ECMO provides only limited leftward PV shift
- Impella partial support: LV still ejects; CO and BP rise → LV end-systolic volume paradoxically rises; PVA not sufficiently reduced
- Impella total support: LV pressure never reaches BP; LV ceases to eject; PVA approaches zero — optimal unloading
- ECPELLA: reduces VA-ECMO-induced PVA while maintaining BP; vasodilator addition further reduces PVA and increases total flow ("total unloading"); excessive decompression risks LV suction → arrhythmias/hemolysis
Device Classification Framework
Four mechanistic categories of percutaneous MCS sources/mcs-ehj-2014 (medium):
- LV pressure unloading: IABP — diastolic inflation reduces LV afterload; modest CO increase (~1 L/min)
- LV volume unloading: TandemHeart (LA-to-aorta) and Impella (transaortic pump) — offload LV by diverting ejected volume
- Biventricular support without oxygenation: modified TandemHeart (RA-to-PA for RV) + LV device in parallel
- Biventricular support with oxygenation: VA-ECMO — full cardiopulmonary support; increases LV afterload
Key Clinical Trials — What the Evidence Shows
EUROSHOCK Registry (n=120 CSMI; Impella 2.5):
- 30-day mortality 64.2%; lactate decreased from 5.8 → 2.5 mmol/L at 48h — hemodynamic improvement but no controlled mortality comparison sources/mcs-ehj-2014 (medium)
ISAR-SHOCK Trial (Impella 2.5 vs IABP; small RCT):
- Impella → higher CI and MAP, lower lactate vs IABP; no difference in mortality, bleeding, limb ischemia, or arrhythmias — hemodynamic superiority without mortality benefit sources/mcs-ehj-2014 (medium)
MACH II study (Impella 2.5 vs conventional in anterior STEMI):
- Significant LVEF improvement at 3 years vs control — suggests long-term cardiac function benefit from early LV unloading sources/mcs-jic-2023 (high)
J-PVAD registry (AMI Killip IV; Impella):
- 30-day survival 80.9% with Impella alone vs 63.1% overall; LVEF improved 35% → 44.7% at Impella explant (P<0.001) sources/mcs-jic-2023 (high)
IMPRESS trial (Impella CP vs IABP; n=48; severe AMI-CS):
- 5-year all-cause mortality 46% Impella CP vs 50% IABP — no significant difference sources/mcs-jic-2023 (high)
Percutaneous LVAD meta-analysis (3 trials; n=100; TandemHeart + Impella 2.5 vs IABP):
- LVAD: higher CI (+0.35 L/min/m²), higher MAP (+12.8 mmHg), lower PCWP (−5.3 mmHg) vs IABP
- 30-day mortality similar (RR 1.06; CI 0.68–1.66); bleeding significantly more frequent with LVAD (RR 2.35; CI 1.40–3.93) sources/mcs-ehj-2014 (medium)
IABP-SHOCK II (n=600; AMI-CS; multicenter, randomized, open-label):
- Intra-aortic balloon pump (IABP) vs control in AMI-CS undergoing early revascularization
- No effect on 30-day all-cause mortality; confirmed no benefit at 6-year follow-up
- IABP does NOT improve outcomes in AMI-CS
ECLS-SHOCK (n=420; AMI-CS; multicenter, randomized, open-label):
- Early VA-ECMO + medical treatment vs usual medical treatment in AMI-CS with planned early revascularization
- 30-day all-cause mortality not lower in ECLS group vs control
- Routine early VA-ECMO does NOT improve outcomes in unselected AMI-CS
DanGer Shock (n=360; STEMI-CS; multicenter, randomized):
- Early microaxial flow pump (Impella CP) vs standard of care in select STEMI-related shock
- Randomized within 24 hours of CS at experienced centers
- 180-day survival improved: HR 0.74 (95% CI 0.55–0.99; P=0.04); 12.7% absolute mortality reduction — first positive tMCS RCT ever sources/cardiogenic-shock-acc-2025 (very high)
- Survival benefit sustained up to 10 years (proportional-hazards ratios over time) sources/cardiogenic-shock-nejm-2026 (very high)
- More bleeding, limb ischemia, and renal replacement therapy in pump group
- Rigorous entry criteria: STEMI-CS only, experienced centers, no risk of hypoxic brain injury
- Only 5% of all CS patients and 32% of STEMI-CS patients in registry analysis meet DanGer Shock eligibility sources/cardiogenic-shock-nejm-2026 (very high)
- Benefit NOT generalizable to HF-CS or broader AMI-CS populations
- Two other microaxial flow pump trials in AMI-CS started; one suspended after DanGer Shock publication
Altshock-2 (HF-CS; n=101; randomized):
- Early IABP placement in acute decompensated HF complicated by CS
- Did NOT improve survival or bridge to heart replacement therapy at 60 days sources/cardiogenic-shock-nejm-2026 (very high)
VA-ECMO 4-trial IPD meta-analysis:
- Individual patient data from 4 randomized VA-ECMO trials in AMI-CS
- No mortality benefit; consistently higher complication rates across all devices sources/cardiogenic-shock-nejm-2026 (very high)
IPD meta-analysis (9 trials; n=1,059; 6-month follow-up):
- Overall: no mortality difference between tMCS and control
- Subgroup benefit: LV-dominant, low hypoxic brain injury risk → HR 0.77 (95% CI 0.61–0.97; P=0.024)
- Complication rates consistently higher regardless of device sources/cardiogenic-shock-nejm-2026 (very high)
ECPELLA (VA-ECMO + Impella Combined)
See concepts/ECPELLA for full detail.
- Rationale: VA-ECMO alone increases LV afterload; Impella counteracts this by draining the LV directly
- Schrage 2020 (n=255 ECMELLA vs 255 VA-ECMO; propensity-matched): 30-day mortality HR 0.79 (P=0.03); benefit only when Impella added within 2h of ECMO (HR 0.76) — late addition >2h was not significant sources/mcs-jic-2023 (high)
- Cappannoli meta-analysis vs VA-ECMO alone: significantly more bleeding (RR 1.45), hemolysis (RR 1.71), limb ischemia (RR 1.43), and RRT (RR 1.54)
- No RCT evidence; all efficacy data observational
Device Complication Rate Comparison (Kapur et al. review)
| Device | Bleeding | Limb Ischemia | Stroke |
|---|---|---|---|
| IABP | 12.9% | 1.5% | 3.1% |
| Impella | 27.7% | 4.2% | 4.9% |
| VA-ECMO | 28.2% | 14.3% | 8.2% |
| Complication burden scales with device size and invasiveness sources/mcs-jic-2023 (high) |
Routine vs Selective tMCS Use
- Routine tMCS in all CS patients is strongly discouraged sources/cardiogenic-shock-acc-2025 (very high)
- tMCS selection should be based on:
- Desired cardiac index (attain CI to improve perfusion when pharmacological support inadequate)
- Device capacity and risk of device-related complications (bleeding, vascular, neurological, infectious)
- Hemodynamic profiling (ventricular involvement, congestion profile)
- LV-dominant STEMI-CS with clinical hypoperfusion/hemodynamic deterioration: microaxial flow pump may be considered
- Most evidence from STEMI-CS; HF-CS largely excluded from positive RCTs — major evidence gap
Escalation Principles
- If undersupported (inadequate CI): escalate tMCS
- If inadequately unloaded: increase current device flow, escalate device (e.g., Impella CP → 5.5), address afterload (LV venting for VA-ECMO), mitigate congestion
- Delays in appropriate tMCS → worsening end-organ perfusion → multiorgan failure and death
- Pulmonary edema + persistent congestion + worsening perfusion/multiorgan dysfunction → team-based escalation discussion
- Stage B patients at highest SCAI escalation risk within 24 hours
tMCS Weaning Protocol
Daily readiness assessment criteria:
- Hemodynamic stability
- Current total vasoactive drug burden (total dose and number of agents)
- Volume status
- Correction or improvement of underlying CS etiology
Weaning approach:
- Stepwise flow reduction: 0.5–1 L/min decrease (e.g., 2 performance levels on Impella) every 2–4 hours
- Success evaluated at each step by: clinical exam + perfusion metrics + echo + invasive hemodynamics (if available)
- Before weaning: advanced HF/transplant consult to determine recovery vs durable LVAD vs transplant
- Acute-on-chronic HF-CS: may require bridge from tMCS with inotropes; prolonged wean often necessary sources/cardiogenic-shock-acc-2025 (very high)
Structured Impella/ECPELLA weaning thresholds (three-step) sources/mcs-jic-2023 (high):
- End-organ adequacy: improved BP + normalized lactate + off pressors + improved RA pressure/PAWP
- RV assessment for VA-ECMO decannulation: RA pressure <15 mmHg AND PAPi ≥1.0 (minimum VA-ECMO flow 1.5 L/min)
- LV assessment for Impella decannulation: PAWP <20 mmHg AND CPO ≥0.6 W (minimum Impella P-level 2)
- Pulse pressure must reappear spontaneously before initiating weaning
- LVOT-VTI increase on echo = LV recovery indicator supporting Impella weaning
- Significant MR at weaning (high PAWP/low CPO): evaluate and consider repair before decannulation
Complications of Large-Bore Vascular Access
- Bleeding: up to 60% incidence in AMI-CS
- Limb ischemia: 4× higher with tMCS; associated with 2× higher in-hospital death
- Prevention: serial limb/access site exam, avoid excessive anticoagulation, attention to catheter angulation/securement, monitor after patient mobilization
- If uncontrollable bleeding or limb ischemia: prompt device removal; ≥12Fr devices should be removed in cath lab or OR
RV Mechanical Support
- Impella RP: intracardiac microaxial pump inserted percutaneously via femoral vein; delivers blood from IVC inlet through pulmonary artery; approved via FDA humanitarian device exemption (HDE) based on RECOVER RIGHT multicenter study sources/cardiogenic-shock-aha-2017 (high)
- TandemHeart RV configuration: used in case series for RV support; limited data
- CentriMag: biventricular surgical support device (requires sternotomy); magnetically levitated rotor; up to 10 L/min; univentricular (LVAD or RVAD) or biventricular configuration; no RCTs — supported by small case series sources/cardiogenic-shock-aha-2017 (high)
Durable MCS and Bridge Strategies
- INTERMACS profiles 1–2 (CS or progressive decline): 38% 30-day mortality after durable MCS implant; profile 1 (active CS) implants declined from 40% (2006) to 12% (2010) — reflects recognition that implanting in active shock carries prohibitive perioperative mortality sources/cardiogenic-shock-aha-2017 (high)
- Bridge-to-bridge strategy: temporary MCS stabilization → hemodynamic optimization → durable LVAD implant; becoming increasingly commonplace; supported by practice guidelines — preferred over direct durable MCS in active CS sources/cardiogenic-shock-aha-2017 (high)
- Heart transplantation: 44% of INTERMACS 1–2 durable MCS implants performed as bridge-to-transplant (BTT); ECMO before transplant low (1.1% of transplants, 2006–2012); concurrent transplant evaluation recommended in all patients assessed for durable MCS sources/cardiogenic-shock-aha-2017 (high)
Common tMCS Device Types
- IABP: counterpulsation; helium-filled 8–9.5 Fr balloon; diastolic inflation augments coronary/systemic perfusion; systolic deflation reduces LV afterload; lowest support level (~1 L/min CO increase); see concepts/IABP for full detail; coronary flow benefit limited to impaired autoregulation states — NOT transmitted past fixed severe stenoses; Benchmark Registry (n=16,909) major complications 2.6%; NRMI-2 showed IABP benefit with thrombolysis but NOT with primary PCI — foreshadowing IABP-SHOCK II null; no mortality benefit in AMI-CS or HF-CS in RCTs; recommended for mechanical complications in European (not US) guidelines sources/cardiogenic-shock-nejm-2026 (very high) sources/iabp-ajc-2006 (medium)
- Microaxial flow pump (Impella): continuous LV unloading; CP model ~4.3 L/min; 5.5 model up to 5.5 L/min; only device with positive RCT (DanGer Shock — HR 0.74; STEMI-CS only); large propensity-matched studies (>100,000 patients) consistently no benefit + higher complications; US Class IIa indication for selected patients sources/cardiogenic-shock-nejm-2026 (very high)
- VA-ECMO/ECLS: full cardiopulmonary support; up to 6 L/min; does not unload LV (retrograde aortic flow increases afterload); ECLS-SHOCK negative in AMI-CS; 4-trial IPD meta-analysis negative; transseptal LV unloading addition showed no mortality benefit in RCT sources/cardiogenic-shock-nejm-2026 (very high)
- TandemHeart: LA-to-femoral; rarely used; up to 4 L/min; 2 small trials, no conclusive clinical benefit
Contradictions / Open Questions
- IABP in HF-CS: Altshock-2 (n=101) negative; routine IABP not supported in any CS phenotype by RCT data — yet widely used
- VA-ECMO retrograde afterload harm: VA-ECMO may worsen LV hemodynamics; LV venting strategies proposed but transseptal cannula RCT showed no mortality benefit — optimal unloading approach unresolved
- DanGer Shock real-world applicability: only 5% of all CS and 32% of STEMI-CS patients meet trial eligibility; positive trial result may be difficult to translate broadly without careful patient selection
- VA-ECMO 4-trial IPD meta-analysis negative: contradicts earlier individual trial data and observational studies suggesting benefit; ECLS-SHOCK cardiac-arrest phenotype contamination may explain null result, but overall evidence does not support routine VA-ECMO
- Inotrope selection: levosimendan failed VA-ECMO weaning endpoint; dobutamine ≈ milrinone; no mortality-reducing inotrope found — clinical practice varies widely without evidence base
- HF-CS evidence void: no positive tMCS RCT in HF-CS; all management is expert consensus or extrapolation from AMI-CS
Connections
- Related to concepts/Cardiogenic-Shock
- Related to concepts/SCAI-Shock-Classification
- Related to concepts/ECPELLA
- Related to concepts/IABP
- Related to concepts/Invasive-Hemodynamic-Monitoring-CS